Looks like no one added any tags here yet for you.
turbinates
warm, humidify, and remove particles from air
epiglottis
protects the airway’s opening
larynx
phonation (voice)
trachea
1st generation of airways
airway generation concept
higher generation = more SA = more gas exchange
external vs internal breathing muscle function
external = inspiratory
internal = expiratory
lung lobes
R: upper, middle, and lower (3)
L: upper and lower (2)
pleurae
double membrane (visceral and parietal) surrounding each lung
visceral membrane
attached to lung
parietal membrane
attached to chest wall
what happens when AIR gets into pleural cavity? is there treatment?
lung separates from chest wall —> deflates —> decreased lung function
no treatment
what happens if FLUID get into pleural cavity?
lungs seperates from chest wall —> breathing trouble
treatment: remove fluid
airways (from biggest to smallest)
bronchus
bronchioles
alveolus
bronchus
big, thick and rigid from cartilage
make mucus via goblet cells
excessive mucus —> asthma
bronchioles
medium size and no cartilage
NO MUCUS (goblet cells)
alveolus
small, single cell wall (thin) allows fast gas exchange between capillaries
type 1 pneumocytes - main structure
type 2 pneumocytes - make surfactant —> decreases surface tension
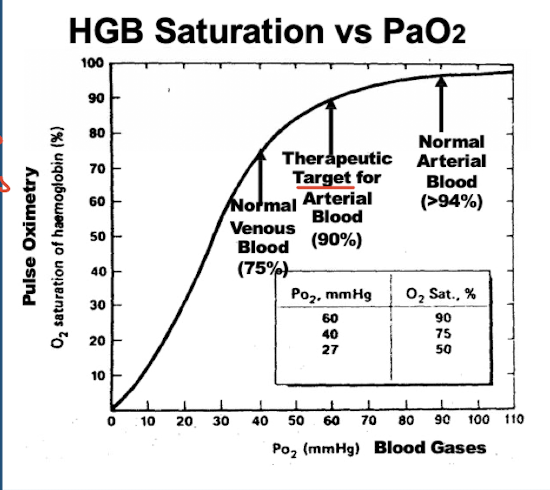
%O2 for normal venous blood, therapeutic arterial blood target, and normal arterial blood
normal venous = 75%
THERAPEUTIC TARGET = 90%
normal arterial = >94%
blue vs red blood meaning
blue = 0% O2 saturation (going to lungs)
red = 97% O2 saturation (leaving lungs)
how would this graph/values shift if person’s in higher altitude?
shift to the left
hyperventilation & causes
aka resp alkalosis
low PaCO2
anxiety, asthma, higher altitude
hypoventilation
aka resp acidosis
high PaCO2
opioids, head trauma
hypoxia
low PaO2
oxygen supplementation treats all hypoxic causes EXCEPT
venous-arterial shunt (abnormal connection between arteries and veins so O2 won’t go to right place anyways)
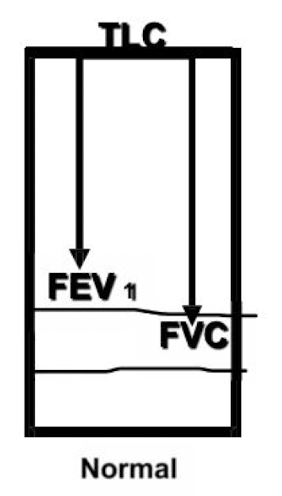
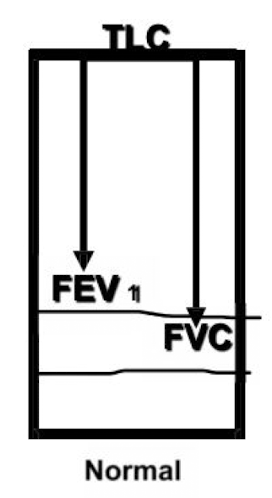
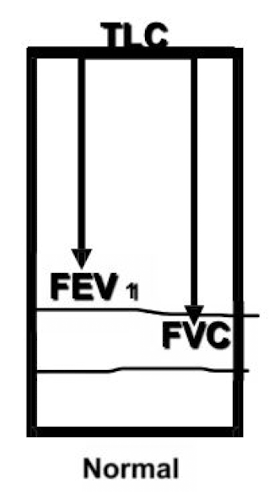
TLC
total lung capacity
fullest volume
FRC
functional residual capacity
volume remaining after a normal exhale
RV
residual volume
volume remaining after max forceful exhale
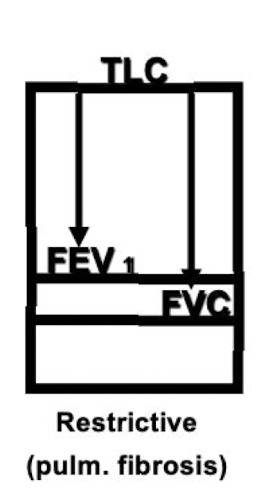
restrictive disease
decreased TLC because lungs can’t fill completely back up
NORMAL FEV1/FVC because both decrease
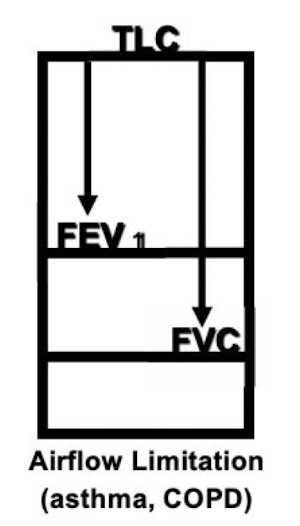
obstructive disease - airflow LIMITATION (asthma, COPD)
decreased FEV1/FVC
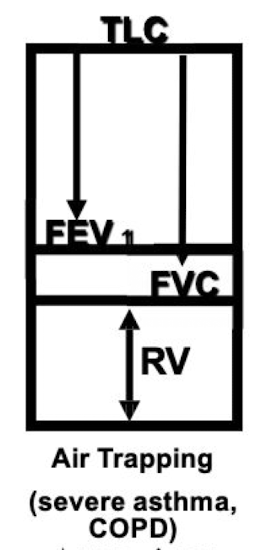
obstructive disease - air flow TRAPPING (severe asthma & COPD)
increased TLC because airways are closed off and very little is exhaled so the lungs get huge
decreased FVC
increased RV
spirometry
detect airway obstruction in asthma & COPD
measures FVC (forced vital cap)
FEV1 = 1st sec of FVC
restrictive disease PFT pattern
everything decreases EXCEPT FEV1/FVC ratio
obstructive disease asthma PFT patterns
normal - increased: TLC, RV, FVC
decreased - FEV1, FEV1/FVC, PEF
obstructive disease COPD PFT patterns
increased: TLC, RV
decreased: FVC, FEV1, FEV1/FVC, PEF