Looks like no one added any tags here yet for you.
Urticaria is treated with
H1 antihistamine and glucocorticoids
Anithistamines
2nd generation of H1 inhibitors - drugs of choice
Prevent mast cell degranulation and inhibit the release of histamine
low sedation
minimal CNS effects → better than 1st gen
Many (not all) have the suffix -adine
Cetirizine
A specific 2nd gen H1 inhibitor
Smooth muscle relaxation (resp sys and vascular muscles)
Decrease capillary permeability
decreases flares and itch
Stabilizes mast cells → Antiinflammation
Safe for pregnancy
Treats things like angioedema, pruritis, etc
Grapefruit decreases absorption and bioavailability!
Topical Capsaicin
Activates and desensitizes TRPV1 → used in the treatment of pruritis
beware, greater than 10 days use depletes substance P stores
Montelukast
Used for seasonal allergies and asthma control
Reduces bronchial reactivity, mucosal edema, and mucous hypersecretion
Potential for serious neuropsychiatric events… beware
Epinephrine
Used in treatment of anaphylaxis
Stimulates Beta2-adrenoceptors in broncial smooth muscle → bronchodilation
Cyclophosphamide
Used in the treatment of Good Pasture Syndrome
Cross-links DNA and RNA, inhibiting protein synthesis and cell replication
aka its cytotoxic
Meant to deplete autoantibody levels
Hydroxychloroquine
Has been used to treat malaria and autoimmune diseases such as SLE (skin manifestations and joint pain) and inflammatory arthritis
MOA unknown
accumulates in lysosomes and increases their pH → inhibiting cell mediated inflammatroy response
Three drugs used in the treatment of SLE
Hydroxychloroquine, Methylprednisolone (a corticosteroid), and Immune suppressants (Rituximab → monoclonal Ab)
Minimum number of drugs to use for HIV
2 (or more)
Can you stop drug therapy for HIV? Why or why not?
Stopping drug therapy will cause the development of resistance due to high mutation rate
Anti HIV classes (7, but 4 major ones)
NRTI - nucleoside reverse transcriptase inhibitors
NNRTI - non-nucleotide reverse transcriptase inhibitors
PI - protease inhibitors
INSTI- integrase strand transfer inhibitors
Fusion inhibitors
Entry inhibitors
PK enhancer
MOA of NRTIs
prodrug enters cell
host cell kinase phosphorylates → activation
active drug competes with human nucleotides for a spot in the elongating DNA chain → prevents HIV viral replications
these drugs cannot eradicate the virus from cells that already integrated pro-viral DNA
Zidovudine
An NRTI for HIV
inhibits mitochondrial DNA polymerase gamma
Side effects
Anemia
Neutropenia
Myopathy
Abacavir
An NRTI for HIV
the ONLY guanosine analoge NRTI
Some are hypersensitive - discontinue immediately, as it can be fatal
Lamivudine and Emtricitabine
The only nontoxic NTRIs for HIV
Tenofovir
Most commonly used NRTI for HIV
only nucleotide analog (all others are nucleosides)
Side effects
Nephrotoxic
Fanconi syndrome
Decreases in bone mineral density with chronic use
Didanosine and Stavudine
NRTIs that cause irreverible sensory neuropathy and pancreatitis
overall avoided
Standard first line treatment of HIV
2 NRTIs with different MOAs (tenofovir-emtricitabine)
1 NNRTI (etravirine) OR 1 INSTI (dolutegravir)
use when patient is pregnant along with the 2 NRTIs
Dolutegravir
INSTI for HIV
Safe for pregnancy!!!
MOA for NNRTIs
chemical substrates bind to the hydrophibic subunit of the HIV-1 reverse transcriptase, causing noncompetitive inhibition
when used along with NRTIs you achieve synergism
NOT active against HIV-2
Nevirapine and Etravirine
NNRTIs that rarely produce life thereating hepatitis or SJS
Autoinducers for metabolism
Efavir and Rilpivirine
NNRTIs given with food
PPIs reduce their absorption
Delaviridine
Rarely used NNRTI thats dosed at 3x per day
MOA of PIs (protease inhibitors)
Peptide like chemicals that target protease enzymes, inhibiting them. This interrupts viral cycle and replication (selective →do not target human proteases)
Active against both HIV-1 and HIV-2
end in -navir
Have poor bioavailablitiy and unbearable toxicity
Ataznavir
PI for HIV that causes Kidney Stones, cholelithasis, and dyslipidemia
Ritonavir
PI for HIV that is often used alongside other PIs
POTENT inhibitor to CYP3A4
increases cholesterol and trigs
MOA Maraviroc
An HIV entry inhibitor
binds to chemokine coreceptor 5 (CCR5), preventing HIV outer envelop protein gp120 binding, fusion, and entry
can cause dose dependent orthostatic HTN
MOA Enfuvirtide
An HIV fusion inhibitor
binds to the gp41 subunit of viral envelope, preventing conformational changes requires for fusion of viral and cell membranes
MOA integrase inhibitors
HIV drug class that is widely used in treatment naive patients due to its excellent tolerability, safety, and antireoviral activity
Suffix -gravir
MOA is essentially preventing viral integration into DNA
-omab
Murine monoclonal antibody
all mouse
Displays the most immunogenecity
-Ximab
Chimera monoclonal antibody
Variable domain is mouse
Constant domain is human
-Zumab
Humanisitic monoclonal Antibody
CDR (complementary determininig region) is mouse
Rest is human
-Umab
Human monoclonal antibody
NO mouse component
Displays the least immunogenicity
Production of Murine mAbs
Conventional hybridoma technology
risk of severe allergic response
Cannot interact with human effector molecules
Production of Chimeric mAbs
Recombinant protein technology
Sometimes the body will make anti-( ) Ab in the presense of these mAbs
Production of Humanized mAbs
Recombinant protein technology
uses only mouse CDRs grafted into human frameworks
Production of Human mAbs
Phage display library
make gene libraries for both Vh and Vl
Use transgenic animals to make the mAbs (but there is no mouse component of these mAbs)
suffix for Fc fusion proteins
-cept
General effector functions of antibodies
Neutralization
Opsonization and phagocytosis
Antibody-dependent cellular cytotoxicity
Complement activation
inflammation
opsonization and phagocytoses
MAC → cell lysis
Naked mAbs
mAbs that act directly when binding to cancer specific antigens and induce immunological response (ex, induce apop, inhibit growth, etc)
Immunoconjugates
mAbs that are modified for the delivery of a toxin, radioisotope, cytokine or other active conjugate
Multistep Targeting
bispecific antibodies that can bind with their Fab regions to both antigen and to a conjugate or effector cell (bringing the two together)
Major targets of mAbs in cancer therapy
CD antigen → CD20 on B cells, CD52
VEGF (vascular endothelial growth factor) inhibitors
EGFR (epidermal growth factor receptor) inhibitors
Inhibitory receptors → PD-1, CTLA-4
Rituximab
Chimeric mAb
Treats chronic lymphocytic leukemia, non-hodgkins lymphoma, transplant rejection, and some autoimmune disorders
Binds to CD20 on B cells, resulting in activation of the immune system to kill B cells via opsonization, ADCC and CDC
Result is decreased B cell levels (cancerous and non cancerous)
ergo, this drug can treat pretty much any condition that involves issues with B cells (ex, Rhemumatoid Arthritis, Myesthenia gravis, etc)
Alemtuzumab
Humanisitic mAb
Treats only Chronic lymphocytic leukemia
Binds to CD52 on mature lymphocytes, but NOT on the stem cells from which they were derived
Ibritumomab tiuxetan
Conjugated Antibody (murine mAb)
IgG1 in conjunction with the chelator tiuxetan, to which a radioactive isotope is added
Treats B cell non-Hodgkin lymphoma in patients who dont respond to other therapy
Recognizes CD20 on cancer cells and delivers radiation that increases antibody killing effect
eg , targets CA cells only!
Bevacizumab
Humanisitic mAb
Inhibits VEGF, blocking angiogenesis
Treats various cancers
trastuzumab
humanisitic mAb
Binds to EGFR (specifically HER2), which plays a role in normal cell growth and differentiation
treats breast, stomach, and esophageal cancer
Drug Targets for Autoimmune disorders
Cytokine or cytokine receptors
Adhesion molecules
CD antigens → CD20, CD2
B7 (with CTLA-4Ig)
Drug TArgets for Allergic inflammatory conditions
Cytokine or cytokine receptors
IgE
Infliximab, adalimumab
Treat Rheumatioid Arthritis
Neutralize the activity of TNF-alpha
Etanercept
Treats RA
TNF-alpha receptor-Fc fusion protein
Abatacept
Fusion protein consisting of the extracellular domain of CTLA-4 and Fc portion, binds B7 and block the interaction inhibiting T call activation
supresses inflammation, decreases anti-collaged Ab production, and reduces antigen specific produciton of INF-gamma
mAbs in Psorasis therapy
Etanercept (Enbrel) -TNFα receptor-Fc fusion protein
Ustekinumab (Stelara)-Neutralize the biological activity of IL-12/23 (responsibe for Th1 and Th17 differetiation - limits type IV HST)
Secukinumab (Cosentyx), Ixekizumab (Taltz) -Neutralize the biologicalactivity of IL-17⍺ (blocks Th17 cells
Brodalumab (Siliq, Lumicef)-Blocking IL-17R
Alefacept (Amevive)-Binds T and NK cells via CD2
Efalizumab (Raptiva)-Direct against leukocyte function antigen-1 (LFA-1)→ interrupt the interaction of LFA with its ligand intracellular adhesion molecule-1 (ICAM-1) (blocks leukocyte migration into tissues)
mAbs in Multiple sclerosis therapy
Ocrelizumab (Ocrevus)-Binds to CD20, deplete B cells
Natalizumab (Tysabri)-Binds to the α4 subunit of integrins
1) inhibiting the migration of immune cells into the central nervous system and
2) inhibiting interactions between integrin and its ligands, thereby possiblyreducing immune cell activation and promoting apoptosis of lymphocytes.
mAbs in Asthma Therapy
Reslizumab (Cinqaero, Cinqair)-Neutralizes biological activity of IL-5
Benralizumab (Fasenra)-Blocking the function of IL-5R⍺
Omalizumab (Xolair)-Selectively neutralizes soluble human IgE
Other applications of mAbs
Anti-SARS-CoV2 mAbs
Abciximab
Target: Platelet glycoproteins IIb/IIIa
Clinical use: Antiplatelet agent for prevention of ischemic complications inpatients undergoing percutaneous coronary intervention
Denosumab
Target: RANKL
Clinical use: Osteoporosis; inhibits osteoclast maturation (mimicsosteoprotegerin)
Palivizumab
Target: RSV F protein
Clinical use: RSV prophylaxis for high-risk infants
Rationale of the Multidrug Approach of Immunosuppression
Multiple drugs with different mechanisms of action will synergistically by targeting different steps
decrease chanves of rejection
decrease in the dose needed for each drug → less side effects
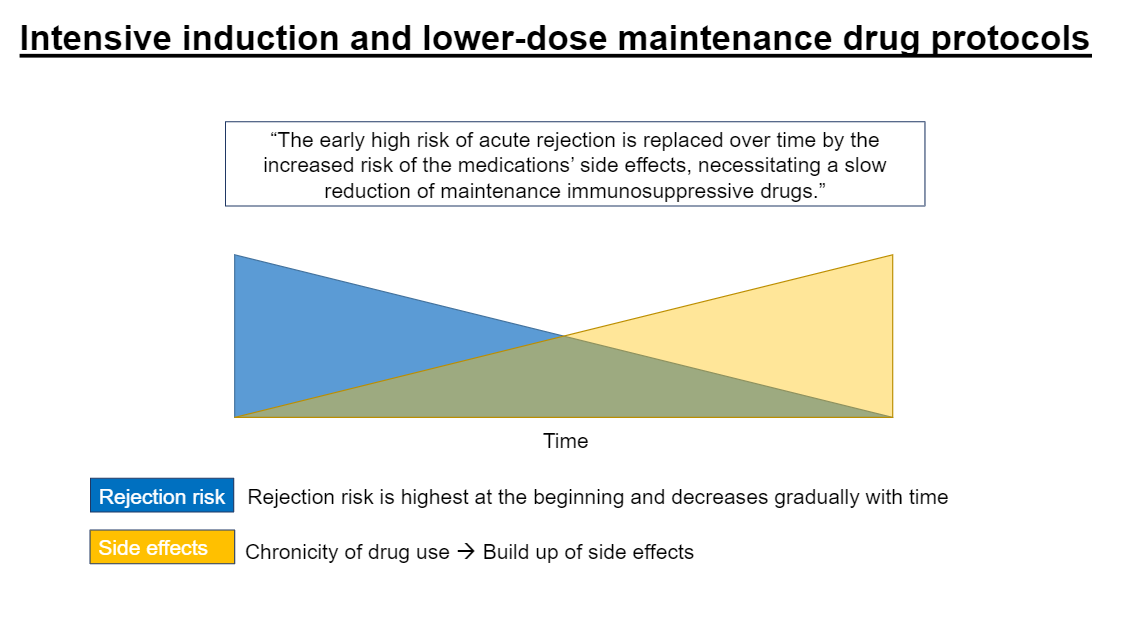
Rationale of Intensive induction and lower-dose maintence protocols with immunosuppressants
Greater immunosuppression is required for early success than to maintain long-term immunosuppression
Rationale of reducing dosage or withdraw a drug if its toxicity exceeds its benefit
Maintence medications are not without side effects, with many of them being dose dependent
Rejection Risk and Side effects with immunosuppressants over time are
inverses of each other
The two categories of induction of immunosuppression
Antibody therapy
T cell depleting agents
Polyclonal Abs
Monoclonal
Non T cell depleting agents
High doses of maintence medication
Antithymocyte globuilin (ATG)
Polyclonal Ab used in immunosuppression
IgG generated from horses or rabbits immunized with human thymocytes
binds to multiple targets on t cells, initially inactivating them, then ultimately resulting in their depletion
Can cause Cytokine release syndrome, esp with the first dose
Treatment for Cytokine released syndrome (which is seen with the use og ATG)
antipyretic → Acetaminophen
antihistamine → Diphenhydramine
antiinflammatory → cortocosteroid
APAP (Aspirin, Ibuprofen) is NOT an
antiinflammatory agent
Alemtuzumab
Monoclonal Ab used in immunosuppression
Binds to CD52
Results in T Cell depletion
Same premedication is given as is for polyclonal Abs (three As…) to prevent cytokine release syndrome
Basiliximab
Non T cell depleting immunosuppressant
Non depleting (monoclonal) antibody against the IL-2R
inhibition of T cell proliferation and differentiation, but NOT depletion
No premedications needed
However, there is a risk for sever acute hypersensitivity
Classes of Maintence Medications for immunosuppression
Calcineurin inhibitors
T cell costimulation blocker
mTOR inhibitors
Antiproliferative/antimetabolites
Corticosteroids
Works before IL-2 production
Works After Il-2 production
Multimechanisitic
Steps of IL-2 production (yes, Dr. S said you need to know)
Stimulation of T cells
increase of intracellular calcium
Activation of of calneurin
Dephosphorylation of NFAT by Calcineurin
Nuclear translocation of active NFAT
Transcripton of IL-2
Talcrolimus
Calcineurin inhibitor
Binds to FK-binding protein 12 (FKBP12)
No IL-2 production
Side effects
Nephrotoxicity
HTN, Hyperglycemia, HLD
Cyclosporine
Calcineurin inhibitor
binds to Cyclophilin (CYP)
No IL-2 production
Side effects
Nephrotoxicity
Gingival Hyperplasia, Hirsutism - specific to this drug only
HTN, Hyperglycemia, HLD
Belatacept
A T cell costomulation blocker
Blocks CD80/86 → preventing costimulation
Prevents production of IL-2 and T cell activation
Everlimus and Sirolimus
mTOR inhibitors
key component of intacellular signaling pathway for cell growth and proliferation
Inhibition of interleukin-driven T cell proliferation
This drug functions AFTER IL-2 is made, just prevents its action
Mycophenolate
Antiproliferative immunosuppressant
Inhibits IMP dehydrogenase → prevents De NNovo purine synthesis
No purines → no lymphocyte proliferation
Azathioprine
Antiproliferative immunosuppressant
Prodrug! Metabolized to 6-marcaptopurine
Fradulent nucleotide that arrests chain elongation and stops lymphocyte proliferation
Prednisone
most commonly used corticosterioid
Exhibits anti-inflammatory and immunosuppressive activity by blocking T cell-derived and APC-derived cytokine expression
Also formes complexes and inhibits other transcription factors such as NFkB
Drugs that need Therapeutic Drug Monitoring
Drugs with a narrow theraputic range and large interpatient variability
For CNIs, CYP inducers/inhibitors can result in
rejection (with induction)
Nephrotoxicity (with inhibition)
For mTOR inhibitors, CYP inducers/inhibitors can result in
Rejection (induction)
Myelosuppression (inhibition)
Most notorious CYP inducers
Anticonvulsants
carbamazepine, phenytion, phenobarbital
St. John’s Wort
Result in transplant rejection due to the failure of drugs like CNIs and mTOR inhibitors
Most Notorious CYP inhibitors
Macrolide ABX
Erythromycin
Clarithromycin
Azole antifungals
Fluconazole
Itraconazole
Ketoconazole
Grapefruit juice
Result in toxicity due to overactivty of druge like CNIs and mTOR inhibitors
Use of Xanthine Oxidase Inhibitors (used for GOUT) alongside Azathioprine (and antimetabolite for immunosuppression) results in
increased side effects (myelosuppression)
Role of TMPT
metabolizes thiopurines to less active compounds
Gentically, lower TMPT activity results in
Greater concentration of thioguanine nucleotides
this results in more side effects with drugs such as azathioprine → myelosuppression
Cyclosporine + Ibuprofen
results in Added nephrotoxicity → Both drugs are nephrotoxic
(Mycophenolate+ Steroid +Tacrolimus) regimen + Live vaccine
BAD idea! Avoid live vaccines, as they are Live vaccines are contraindicated in immunocompromised patients due to the risk of severe systemic disease
(Mycophenolate+ Steroid +Tacrolimus) regimen + Inactivated vaccine
OK to do! Non-live vaccines can be administered in patients on immunosuppressants after the immune system recovers from induction. However, lower response is to be expected. It is always better to complete the vaccinations prior to transplant/immunosuppression.
Everolimus + Phenytoin
Results in Risk of rejection → Phenytoin is a CYP inducer → decrease severolimus concentration (remember mTOR inhibitors are CYP substrates) → risk ofrejection