How do we generate speech?
Preparatory breath-
inhale,
lower diaphragm, and
lungs expand
Controlled exhalation-
Rest breathing- we don't do anything to control the breathing
Controlled breathing- for speech, we need control and to generate a certain pressure
Volume
Pressure
Flow
What are the two sections of the respiratory system and what do they consist of?
Upper respiratory system
Nasal, oral and pharynx
Area that is the resonator
Space above the vocal folds
Lower respiratory
Anything below the level of the vocal folds
Bronchial system and the lungs
Rib cage and the diaphragm
Bronchial tree
Trachea, bronchi, bronchioles, alveoli, lungs
Label the lower respiratory system top to bottom
Thyroid cartilage
Cricoid cartilage
Trachea
Tracheal cartilage rings
Open in the back and look like a horseshoe
Primary bronchi
Secondary bronchi
Tertiary bronchi
Bronchioles
Terminal bronchiole
respiratory bronchioles
Alveoli
What is speech breathing?
Speech breathing- actively letting the air out of you in a systematic way to control the air going out of you that actively engage rectus abdominis
What are the roles of the abdominal muscle?
1. Flex or bend of vertebral column
2. Enclose and support abdominal contents
3. During respiration, Displace abdominal contents and increase abdominal pressure and Draw ribs down
What separates the internal and external intercostal muscles?
Fascia
What is pleural linkage?
Means by which the lungs are linked by the thoracic wall (rib-cage)
Parietal pleura lines the inner thoracic cavity
Visceral pleura lines the outer lungs
What is the space between visceral and parietal pleura?
Intrapleural space- Fluid inside that fills up the space and it is filled with a fluid to help reduce friction. Keeps the lungs inflated, moving, and negative pressure holding them together. This is the reason behind the movement of the lungs. Also called surfactant
How is pleural linkage accomplished?
Outer surface of lungs covered by thin sheet of membrane visceral pleura
Inner surface of thorax and superior surface of diaphragm covered by parietal pleura
Between the two pleura is the intrapleural space
Fluid filled negative pressure interface links the two together
The difference between pressure inside the lungs and the intrapleural pressure is known as what?
transpulmonary pressure (Under normal conditions Transpulmonary pressure is always a positive value, Small amount of negative pressure should not be more than their lungs)
Explain to me by what we mean by resting expiratory level
The neutral position of the lung thorax unit, occurs right before you take your next breath
At the mechanically neutral position of the lung thorax unit
1. Attached muscles are neutral (physical position)
2. To move past REL you have to activate muscle effort
(To get away you have to activate external intercostals and engage the abdominal muscles)
3. ***38-40% of your vital capacity ***
4. Ambient and alveolar pressure are equal
Why do I have to expend muscle energy to get air in me?
Have to overcome 3 resistances
1. Resistance to airflow through respiratory airways
2. Resistance to deformation of respiratory tissues
3. Elastic recoil of lung-thorax unit
Explain inhalation
At first atmospheric pressure = alveolar pressure. Alveolar pressure needs to become more negative, to do this 1. The diaphragm contracts which makes vertical dimensions of the lungs larger 2. External intercostals contract which pull the rib cage up and out makes the back 3. Lungs attached gain volume and therefore creates negative pressure relative to atmospheric pressure so air rushes into the lungs to make atmospheric and alveolar pressure equal again. Requires active applied muscle force.
Why is the top of inspiration kinda similar to atmospheric pressure?
Because you cannot get more air in
Explain exhalation
To exhale we must get P alveolar to be greater than atmospheric pressure. Intercostals relax, diaphragm goes back up which decreases the volume of the thoracic cavity. Elastic recoil gets the air out of us. As volume decreases, alveolar pressure is greater than the atmospheric pressure and air rushes out of the lungs. Passive- recoil force of lungs thorax unit. Happens with exhalation, we just let go. Brings you back to REL
What are the Four forces that cause the thorax and lungs to recoil?
1. Gravity- naturally act upon us to pull the ribcage down
2. Relaxation of the contracting muscle- Including the diaphragm and intercostal muscles, because they are elastic they want to be returned to their shape after being displaced from rest. Diaphragm will go back to its dome shape
3. Elasticity- Of the respiratory tissues and lungs. They want to return to their relaxed state
4. Torque of the ribs- costal cartilage of the ribs untwist as they return to their original shape. Cartilage is a little elastic so you can move it around. Is a passive thing once you let go, their “snapping” back in place after twisting up
When do passive forces take place?
Quiet breathing
What is a typical respiratory cycle; describe the graph.
A- the amount of lung volume change (measured in liters of air). 0 at rest before you take a breath in. As you breathe in, lung volume increases. Lung volume is increasing due to the contraction of the inspiratory muscles. Happening at the same time as B and C. Increase in lung volume
B- inspiratory flow (measured in liters per second) 0 is at rest. Flow is air moving in, talking about it at B in terms of negative alveolar pressure due to the increase in alveolar lung volume (negative flow inward) Decrease in alveolar pressure, resulting in an inward flow of air
C- flow inward is happening because of the change in alveolar pressure. Lung volume is bigger so they become more negative in terms of the pressure outside (atmospheric). Inward flow of air
G- the end of the inspiration. Not REL because you are at a higher volume then you are at rest. Reached the end of the inspiration, cannot take more air in, no longer moving. Pressure equals atmospheric pressure (but not REL). Lung volume is not changing. Flow has stopped. Alveolar pressure and airflow rate return to 0. Pressure is unchanging
D- lung volume is decreasing during expiration
F- pressure is increasing, decreasing lung volume results in positive alveolar pressure that vary overtime but remains positive throughout expiratory phasez
E- positive pressure is going out (positive flow is going out). Positive alveolar pressure results in a positive (outward) flow of air that varies in magnitude with alveolar change
At the end of expiration, alveolar pressure and flow rate are back to zero
What are the active muscles of expiration?
Abdominal muscles and the internal intercostal muscles
What is forced breathing driven by?
the need of O2 and to get rid of CO2
What are volumes?
Single non-overlapping values that are discrete measures
What are capacities?
Typically made up of two or more volumes; measured in cubic centimeters or liters/milliliters
What does EEL stand for?
End expiratory level, the end of inspiration
Define resting expiratory level? REL
The rest position or the neutral position or the equilibrium position of the lung thorax unit. Reach REL when P alveolar is equal to atmospheric pressure. At the end or beginning of inspiration or exhalation. 38-40% of an individual’s vital capacity.
What is tidal volume? TV
Volume of air inspired and expired during any respiratory cycle. 0.6-0.75 liters. Dependent on the activities benign performed, age, and gender.
What is vital capacity?
A combination of inspiratory reserve volume, tidal volume, and expiratory reserve volume. It is the max amount of air that can be expired after a maximum inspiration. Typically 5 liters. It is the maximum amount of air, or the amount of air let out after your deepest breath in. Depends on age and size.
What is inspiratory reserve volume? IRV
Maximum amount of air that can be inhaled from the end expiratory level, or the amount of air that can be inhaled above the tidal volume. The amount of air that you can access if you need it. 1.5 to 2.5 liters
What is expiratory reserve volume? ERV
Maximum amount of air that can be exhaled from end expiratory level, or the amount of air that can be exhaled below tidal volume. 1 to 2 liters.
What is residual volume? RV
Amount of air remaining in the lungs after maximum expiration, this is what keeps your lungs inflated. 1 to 1.5 liters
What is functional residual capacity? FRV
Volume of air in lungs and airway at REL or EEL. Is the expiratory reserve volume plus the residual volume. Is 2.5 to 3.5 liters
What is the inspiratory capacity? IC
Amount of air that can be inhaled from EEL. Is the tidal volume plus the inspiratory reserve volume. Is 2.5 to 3.5 liters
What is the total lung capacity? TLC
The total amount of air lungs are capable of holding. Volume of air in the lungs and airways following maximum inspiration. Is made up of the inspiratory reserve volume, the tidal volume, expiratory reserve volume, and the residual volume. 5.0 to 6.0 liters.
REL is what percentage of the vital capacity?
30-40%
What percentage of vital capacity is taken up by life breathing and where in accordance with REL and VC does it take place?
10% VC, Takes palace at a level above REL to 50-55% of VC
What percentage of vital capacity is taken up by speech breathing and where in accordance with REL and VC does it take place?
20% VC. Takes place above REL and runs midrange of total vital capacity of 55-60% of VC for speech breathing
What percentage of vital capacity is taken up by loud speech breathing and where in accordance with REL and VC does it take place?
40% VC, Starts at around 80% above VC, want to start high and go down
What percentage of vital capacity is taken up by child speech breathing and where in accordance with REL and VC does it take place?
35% VC, Takes up more of total vital capacity compared to adult life breath. Use more of their lungs and go all the way down below REL and continue to talk to where they are operating inefficiently and going below expiratory levels and engage expiratory levels
Where do most breathing activities take place?
Above REL
How much of VC must be used in order to be able to produce speech?
Must be 20% of vital capacity and we want to see it occurring at 40-50 % of VC. (Around 40-60% of total vital capacity)
Compare breathing for life to breathing for speech. What are the differences? (hint: there are 5 main ones.)
1. Intake location
BFL- nose
BFS- mouth
2. Ratio of inhale and exhale time
BFL- 40/60% and exhalation lasts around 2 seconds
BFS- 10/90% and exhalation can last up to 25 seconds because there is more voluntary control, is more complicated, and has more things to manipulate
3. Passive or active forces
BFL- passive exhalation as muscles of the thorax and diaphragm relax. Used forces of torque, elasticity, and gravity)
BFS- active exhalation thoracic and abdominal muscles contract to control recoil, the rib cage, the diaphragm, and the internal intercostal to control air going out of you in a steady fashion
4. Volume of air and vital capacity
BFL- volume of air is 500 cc and is 10% of the vital capacity
BFS- volume of air varies depending ont he strength and loudness along with varies the vital capacity which is typically 20-25%
5. Chest wall position
BFL- abdomen is displaced outward relative to the rib cage
BFS- abdomen displaced inward relative to the ribcage. Allows to take air in and to be able to make quicker breaths during speech. Also affects how much volume we have for air
Name 3 types of breathing for speech; describe their lung volumes and vital capacities.
1. Connected speech- Rarely started from lung volumes at or below REL. Usually start 40 to 60% VC
2. Loud speech- Usually initiated from 60-80% VC terminates at higher lung volume. More air, more lung volume. Two steps: 1. we are going to breath in until we reach 60-80% of total vital capacity and start speaking, 2. Go down to about 40% and then breathe again. Much higher than the 5-10 (at least 20 if not higher)
3. Soft speech- Initiated at lower %VC but still above REL. Might initiate at 40 or a little above . Terminates at REL
What does breathing for speech depend on?
The positive pressure that is generated as air exits the lungs
What are the two ways positive pressure is created?
1. Passive forces during exhalation (recoil). Take a breath in and recoil out (passively)
2. Active muscle effort. Breath in and push with belly and push with chest (active muscle effort)
What are the four restoring forces that cause the thorax and lungs to recoil?
1. gravity pull rib cage downward
2. relaxation of the contracting muscles, including the diaphragm (returns to dome shape)
3. elasticity of the respiratory tissues and lungs
4. torque of the ribs (ribs untwist as they return to their original positions
What is the amount of positive pressure needed for speech?
5 to 10 cm H2O
_ for _ is a ratio that someone has a really good shot at being able to maintain speech
5 for 5 (5 cm of water pressure for 5 seconds)
What does the pressure relaxation curve show?
The kind of pressure we can generate based on the kind of vital capacity. It also shows the negative pressures. It shows what happens when we relax at a specific vital capacity.
What do you have to do in order to move away from REL? Also what you need to generate pressure.
Engage muscles
What happens anytime you increase the volume in the lungs?
You have negative pressure created
What is this graph, what does it show, and explain each letter point.
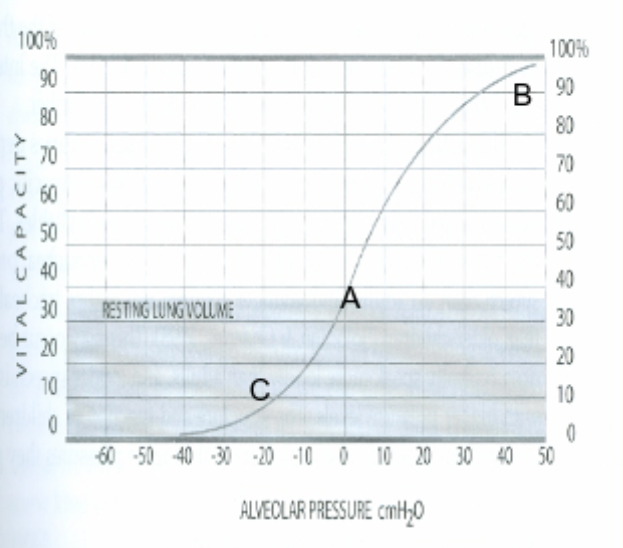
-B- Shows how once the lung thorax unit is moved to a higher lung volume (B), recoil will generate positive alveolar pressure
-C- if the lung-thorax unit is moved to lower volumes (c) then recoil will generate negative alveolar pressure
- this is the relaxation pressure curve and it represents the passive forces
generated due to the elastic properties of the lung-thorax unit
Looking at the graph above, what kind of pressure can I generate based on the vital capacity I am at? If I am at 50% vital capacity, what pressure do I generate? Is this enough to produce speech?
Around 5 cm H2O. Yes it is.
Explain: True or false: it is possible to generate more alveolar pressure (whether positive or negative) than it is possible due to passive forces
True, this is accomplished by applying additional muscle effort to further expand or contract the thorax
Fill in the blank: REL is when we are at _______.
Neutral
Why does a bigger vital capacity mean negative pressure? (above REL)
Bigger = negative (pushed out and relaxed and it made us breath in and give us a bigger volume means we have to go into the negative because bigger volume generates negative pressure in the lungs)
What is the vocal tract a series of?
Valves, when we speak we are valving the airstream
How do we produce sustained phonation? What happens to pressure, volume, and flow?
Pressure- the power for speech
Subglottal pressure rises to a level appropriate for demand of sustained utterance. This level varies depending on the demand (intensity). This remains steady throughout utterance and falls back to atmospheric upon completion of utterance.
Airflow-
Airflow rises from 0 once utterance begins. It is maintained at a steady level throughout the utterance. It falls back to 0 once the utterance is complete.
Lung volume- the volume inside the lungs in percent of Vital capacity
Lung volume rises to maximum prior to inflation of phonation. Lung volume starts to drop as air is used to produce vowel sound. IT then decreases until no air is left for phonation.
What are the pressures that need to be controlled in order to produce the required amount of positive pressure that is needed for speech? Two things:
1. Checking action- of the inspiratory muscles which regulate the reate the thoracic cavity and lungs return to their original positions (recruits muscles to slow the deflation rate)
2. Abdominal muscles contract to continue exhalation below the resting expiratory level
At each point in the relaxation pressure curve talk about the kind of pressure that you would generate at the point and whether or not there is muscle energy involved.
A- pressures due to recoil exceed pressure requirements of an utterance. Net inspiratory muscle effort is added to recoil in a checking or breaking action. Has more than enough pressure for speech. engage inspiratory pressures to slow it down so we do not use the air too fast. More than enough to produce speech, over 5-10 cm H2O.
B- at this point recoil forces generate alveolar pressures just sufficient to meet utterance demands. No additional muscle effort is required. Almost to REL. Inadequate pressure. Start engaging expiratory muscles to help maintain what we need. Cannot rely on recoil.
C- pressures due to recoil fall below pressure requirements of utterance. Net expiratory muscle effort is added to recoil to meet pressure demands. Negative pressure then uses recoil to let go. Will generate negative pressure from the volume increase. When you are below REL so you let go and are going back up to REL.
What does this graph show?
Shows muscle activity during sustained phonation. Negative muscular pressure implies inspiratory muscle effort. Positive muscular pressure implies expiratory muscle effort.
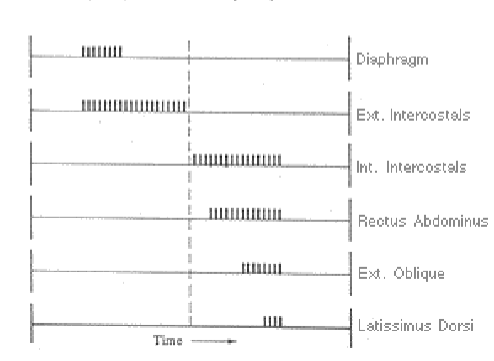
What does this graph show?
Depicts temporal activity of some respiratory muscles during sustained vowel. The diaphragm and external intercostal are shown to be active during phase in which inspiratory or breaking action is required to offset excessive +recoil forces. At recoil pressure no muscle effort is required. Expiratory muscles shown to be active during phase in which recoil forces are insufficient to meet pressure demands of utterances. Can use inspiratory and expiratory muscles simultaneously. Not uniform, varies in people
What does this graph show?
The relaxation curve in terms of zones. Shows the relationship between recoil forces, expiratory muscle effort and inspiratory muscle effort varies depending on the nature of the sustained utterance task. (3. For loud utterance, less inspiratory muscle effort is required and through a shorter vital capacity range. However, more muscle effort is required through a greater vital capacity range. Vital capacity 60-80%, pressure = 20 cm H2O) (1. For a soft utterance the opposite takes place. Greater inspiratory muscle effort is required at higher lung volumes and through a greater lung volume range. Vital capacity 45%, pressure = 3 cm H2O) (2. Less expiratory muscle effort is required at lower lung volumes and through a smaller range of lung volumes relative to the normal utterance. Vital capacity 55%, pressure = 5 cm H2O)
Where are kids typically around in terms of water pressure for speech?
Kids are always around 35-45 of water pressure because they are little so they generate great pressure
The pattern of muscle activity (and the pressures generated) for speech exhalation depend on what five things?
1. Intensity
2. Length of utterance
3. Emphasis
4. Where stress is placed (stressed syllables last a little longer, little louder, and are a little higher in pitch)
5. Age
What are the differences between quiet breathing and speech breathing?
1. Breaths per minute
QB- 12 or more breaths per minute
SB- breathing frequency decreases
2. Ratio of inspiration to expiration
QB- Amount of time for expiration approximately equal to inspiration
SB- inspiration more abrupt (quicker) while expiration lengthened (extended)
3. The state of the breath
QB- steady efficient state
SB- Not like sustained phonation (not like the 5-10)
What is steady in speech breathing?
Trick question, nothing. Everything is constantly changing. There are no steady state pressures, air flow rates, or resistances. Changes are often rapid and large.
What do changes in speech breathing depend on? Explain each.
1. where speech events are measured. Pressure and flow changes on part of the utterance (needs are going to be different). Whether at the beginning or middle. Dictates connected speech.
2. phonetic factors. How the sounds are produced rather than placement. How am i producing this sound and how do those affect things across the board
3. prosodic factors. Include stress, intensity, pitch, rate, duration
What does conversational speech involve more of?
Conversational speech involves more frequent demands for rapid changes in muscle effort, this means more expiratory effort and inspiratory breaking.
What is the difference between breathing for sustained phonation for isolated vowels and breathing for conversational speech?
For sustained phonation we maintain a constant pressure and flow while volume is decreasing at a constant rate. Inspiratory and expiratory muscles are active throughout (different muscles active at different times)
For connected speech a steady outflow of air is also still needed to support the utterance. Has additional demands: More variability in pitch, loudness, rate of speech, duration of utterance, linguistic stress.
What are the advantages of the positioning of the rib cage and the abdomen during connected speech
Position: Abdomen smaller (pulled inward), rib cage larger (held outward) than during relaxation. Abdominal wall is going to push the diaphragm upward in this position.
1. Quickness- This allows the diaphragm to make quick, strong contractions and facilitates quick inspirations (makes quick contractions, quick exhalations and inspirations).
2. Changing pressures- This position helps us to meet changing pressures for speech (stress in speech), and lets you address all of the lung volumes needed for speech,
3. Promotes continuity and movement- Helps to promote continuous movement of lung and rib cage to generate necessary changes in lung volumes. Which result from changes in rib cage movement and diaphragm movement so this position allows for all the movements.
4. This position is efficient. It creates a stable base and support the lung-thorax unit for pleural linkage.
How does a person’s lung volume when speech is initiated affect their chest wall?
At typical lung volumes the respiratory structures can passively generate Palv of 5-8 cm H2O, thus chest wall doesn’t need much setting up for speech
At lower lung volumes so the chest wall will need to quickly make muscular adjustments to begin speaking
What is the initiation and termination of a low, typical, and high lung volume?
Low lung volume/VC- Initiation: 19% VC, termination: 14% VC, Hard to talk like this. You’ll get away with it but have to work really hard
Typical lung volume/VC- Initiation: 51% VC, termination 45% VC, Hangs out at those higher levels So we can take advantage of recoil
High lung volume/ VC- Initiation : 89% VC, termination 80% VC
What describes a good voice quality?
Mid range volumes all the time, and Good clear voice with no effort
What does the amount of muscle effort required at given instant during speech depend on?
Amount of muscle effort required at given instant during speech depends on Palv demands and recoil forces available. Conversational speech occurs between 40 - 60 % VC and recoil pressures vary between 0 - 10 cm H2O here. When you add abdominal effort as a possibility, an average of 5-8 cm H20 is required during speech.
Describe to me some of the other influences on speech breathing
Breathing for speech is also influenced by where I am going to breath for linguistic message, the complexity of speaking task -> deeper breath for when we have to say something for a long time or talk a lot of words, the type of phoneme because it produces different flow that influences your breathing, whispering you are going to terminate your breath at a lower lung volume, loudness will make you breath in more deeply
Describe how the complexity of a speech task affects speech breathing.
The more complex the task the smaller the number of syllables per breath group, the slower the speaking rate, and the greater the average volume of air/syllable
Describe how the type of phoneme in a speech task affects speech breathing.
Voiceless stops and fricatives need a higher flow vs voiced stops and fricatives need a lower flow
Describe how whispering in a speech task affects speech breathing.
Terminate breath groups at lower lung volumes, fewer syllables per breath group, and more expended per syllable
Describe how the loudness of a speech task affects speech breathing.
Greater volume of air in a shorter period of utterances vs soft utterance begin at lower lung volumes
How is the chest wall shaped during speech?
Abdomen smaller, rib cage larger than during exhalation
Where/what approximately is the volume during speech?
Midrange of vital capacity, Approximately twice the volume of quiet tidal breathing
What are the linguistic breaks timed with?
Inspirations are timed with naturally occurring breaks
What are the different lifespan terms associated with speech breathing as we age.
emergence
refinement
adaption
what is emergence?
Birth to 3 years of age. At this stage changes in lung volume are accomplished mostly by displacing diaphragm. This is because your bones are still developing so you do not have the torque generation because the costal cartilages are not developed yet. The passive forces that collapse the lungs are very great. Airways are small and haven't grown
What is refinement?
Time when speech has begun to emerge. Age 4 and up. Things are growing in general. Speech is not sufficient
What is adaption
Lung width, length, and total capacity continues to grow until ages 14-16. Efficiency in breathing for speech becomes more adultlike. Occurs with physical growth and linguistic maturity. Language is more complex. Starting to make jokes and manipulate people.
How is children's speech different compared to adult speech?
They produce speech using a higher percentage of lung (vital) capacity. Smaller airways generate higher pressures for speech and operate at higher speaking pressures as compared to adults. They inhale more deeply and begin speaking at higher lung volumes and then end utterances at lower lung volumes (below EEL). Go below end expiratory levels and REL. They make a lot of revisions and therefore are less efficient, and are less fluid, have more hesitations, and use more pauses and fillers. They do not rely on rib cage movement.
How does speech change after adulthood into old adulthood?
Ossification and calcification of costal cartilages begins. There are changes in thoracic shape (more convex). Force and rate of respiratory muscle contraction decrease. There is progressive loss of alveolar surface tension and pulmonary capillary blood volume. Lung size decreases. There is a decrease in chest wall compliance. Recoil pressures of lungs are affected in the mid volume range. They have lower VC, ERV, and IRV and increases in RV and efficiency is poorer. Changes are uniform and gradual till 60-70, then the effects vary more. The speed of transmission slows down and so does muscle action. Alveoli loses surface tension, which means lungs lose size too.
How do position and posture affect how we breathe?
In an upright position at rest gravity acts in the expiratory direction on the rib cage, and in the inspiratory direction on the abdomen. However, in the supine position at rest gravity acts in the expiratory direction on both the rib cage and the abdomen. This will influence the relaxation pressure curve and REL.
Why do I always want to be above REL when speaking
Because it is easier to speak. This is because you take advantage of recoil when you start at REL. It takes more muscular effort to speak. You are above REL and do not need to engage muscles as much.
Describe one instrumentation, tell me what it measures, explain to me why it is important?
Choose one-
Pulmonary Function testing (PFT)- Direct measuring of lung volume and flows, Good for measuring vital capacities and volumes
Spirometry- Amount you push up is equated to your volume, Good for measuring vital capacities and volumes
Head out body plethysmograph- Measures volume based on pressure and flow
Respiratory inductance plethysmography (RIP)- The cross-sectional areas are measured (chest and abdomen). As you breathe in and out you are going to change the shape of the wires and the coiling and the plethysmography. It measures volume.
Linearized magnetometers- Look at the changes in the fields of the magnets. Change in voltage which relates to a change in volume. This is useful when they cannot blow to do a pulmonary function test. Measures volume
U tube manometer- At rest water in both columns of the manometer are equal height. As you breathe you will displace the water. Related to centimeters of water pressure you create by blowing. Measures oral pressure
Phonatory analysis system- Measures intraoral pressure. Is a closed system. Related to what we are doing with the articulators during the vocal folds. Can also measure airflow.
Pneumotachometer- Used to measure airflow. Can have this right over the mouth or nose during speech tasks.
What is FEV1?
Amount of air that can be exhaled forcibly in one breath in 1 second.
What is FVC?
Amount of that can be forced after a maximum inhalation
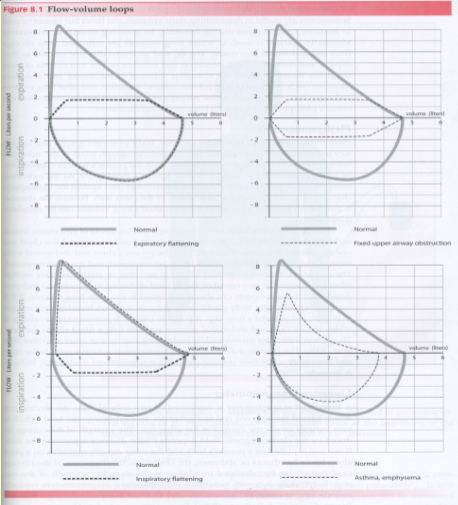
What is a flow volume loop? Explain the graph and what they mean.
A flow volume loop is a presentation of what is happening when we inhale and exhale and compares it to norms to show different lung pathologies and how they act. Segments 1-top left, segment 2-top right, segment 3-bottom left, segment 4-bottom right.
Segment 1- expiratory flattening: a person can breathe in well but can not exhale well.
Segment 2- fixed upper airway obstruction: has a hard time with inhalation and exhalation.
Segment 3- inspiratory flattening: can exhale well but cannot inhale well
Segment 4- asthma, emphysema: slightly below normal for both inhalation and exhalation
What measures respiration based on flow? What about pressure? What about volume?
Flow- Pneumotachometer, Phonatory analysis system
Pressure- U tube manometer, Phonatory analysis system
Volume- Spirometry, FEV1, FVC, Pulmonary Function testing (PFT), Respiratory kinematic analysis, plethysmograph, Respiratory inductance plethysmography (RIP), Linearized magnetometers
What are our expectations for flow rate?
Flow rate tells us if they have a compromised respiratory system. If they meet the goal they are still good for speech.
What factors affect flow?
Manner (what phoneme is produced), age, and Neurologic diseases (for example Asthma and Bronchitis)
What are the effects of excessive compliance and loss of compliance?
Compliance- volume changes produced by a unit of pressure change. More compliant = easier to move, when compliance increases very quickly pressure will decrease and elastic recoil decreases. Less compliance = stiffer = more resistant to movement, and cannot be easily moved to a vital capacity.
What is excessive compliance?
Conditions where we are way stretched out. Creates a loss in pressure. Steep curve. If you have this as soon as you fill up to vital capacity you immediately move to a force exhalation to reach the pressure you need in the system. Closer to REL = exerting effort = forced exhalation. Try breathing out really hard. Hard time generating pressure
What is loss of compliance?
Everything is stiff and not as easily moved. When you take a breath in you never get to a 100 % Vital capacity. Your ribcage is driving everything. Loss of elasticity. You can only get to about 40% of vital capacity. Elastic recoil you are so stiff so you are going to snap back instead of a nice easy movement. Loss of compliance = reduced vital capacity. You can generate larger pressure for a larger amount of time. Take breaths more frequently and cannot depend on recoil.
What is Dyspnea and stridor.
Dyspnea- Discomfort in breathing or shortness of breath
Stridor- Audible inspiration and expiration; Obstruction of airway collapsing in on itself