Looks like no one added any tags here yet for you.
It is normal to experience ___________ cognitive and brain changes with age. a.k.a _______________________
some mild, subtle cognitive changes (healthy and optimal)
Some individuals experience cognitive and brain
changes that are _______________ in nature. These cognitive changes cause __________ in ADLs or IADLs.
Often times due to a _______________________________________ process.
moderate to severe, declines, pathological or
neurodegenerative
Our goal as medical professionals is oftentimes to
distinguish b/w _________ vs. _____________ disease states.
normal, pathological
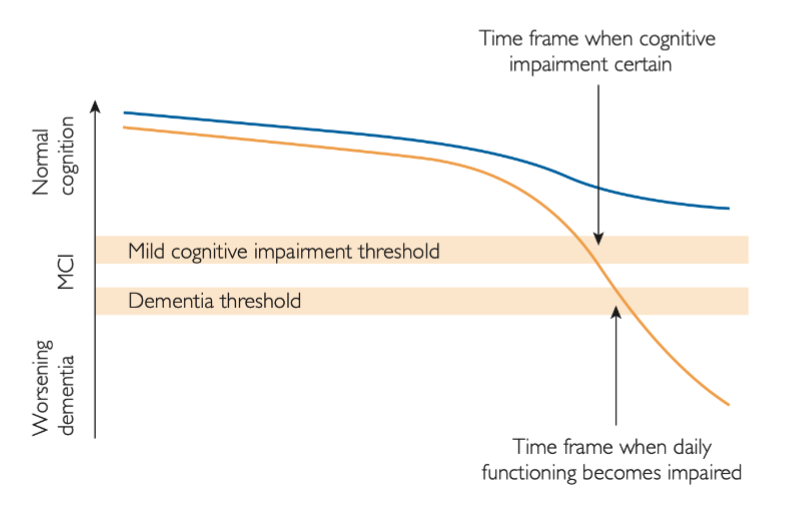
What does the blue line show?
What does the orange line show?
Blue shows trajectory of person destined to die nondemented (unimpaired)
Orange shows trajectory of person destined to develop dementia (impaired)
What are some questions you can ask yourself when assessing a person for dementia?
• Is this person experiencing a decline in cognitive
functioning?
• Is this cognitive change mild, moderate, or severe in
nature?
• Is this cognitive change indicative of impairment?
• Is this cognitive change affecting their everyday
functioning?
• Is this an isolated cognitive issue or are multiple cognitive domains affected?
• What is causing this cognitive change?
We use ___________ data to understand the difference
between normal and impaired cognitive scores.
normative
We are interested in whether someone performs
______________________ the expected average score in a cognitive test to a large sample of older adults.
significantly below
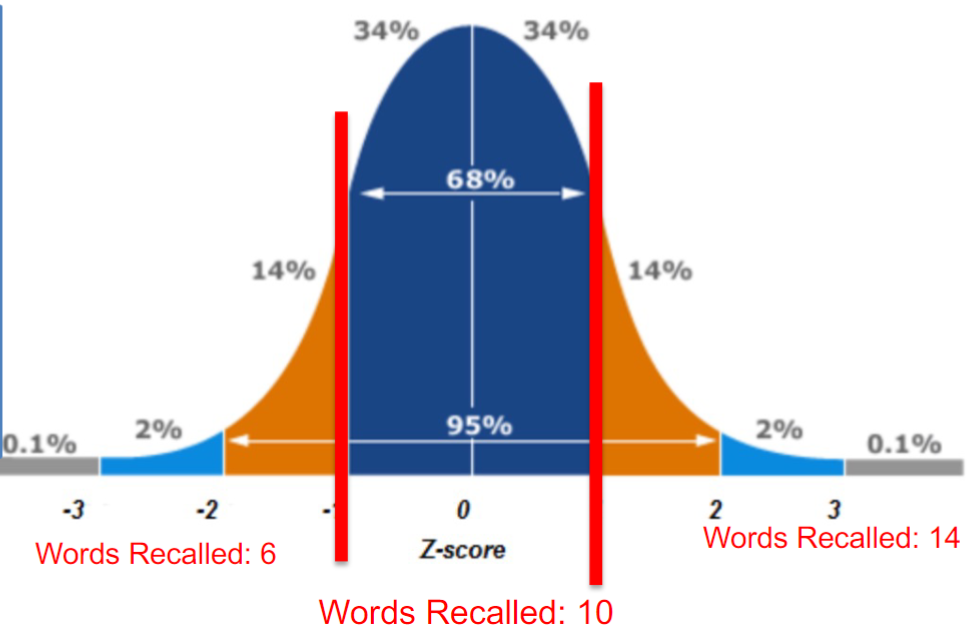
Explain the bottom portion of this graph
There is a small subset of 20 year olds in the population that will recall fewer than 10 words.
These individuals are BELOW the mean.
This is statistically less common and these individuals are in the BOTTOM 16% of the sample.
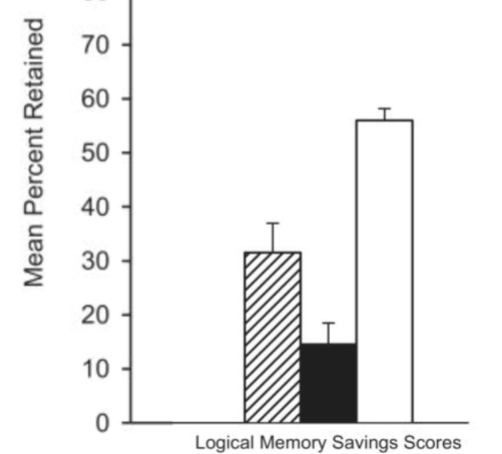
Do different types of dementia have the same patterns of impairment across tests?
No
Which pillars match to the corresponding types of dementia?
AD
DLB
NC
Dementia with Lewy Body - striped
Alzheimer’s Dementia - solid
No Cognitive Aging - white
What are the different types of dementia and their prevalence among the population?
Alzheimer’s - 60-80%
Lewy Body Dementia - 5-10%
Vascular Dementia - 5-10%
Frontotemporal Dementia - 5-10%
Others: Parkinson’s, Huntington’s
Mixed Dementia
Define dementia.
A syndrome associated with changes in thinking, emotions, & behavior that impair an individual’s capacity for independent living
What is a syndrome?
A constellation of signs and symptoms that often occur together
What is a sign?
Objective measurable phenomenon observed by another person (e.g., forgetting items on the grocery list; cognitive test scores)
What is a symptom?
Subjective experience of individual affected (e.g., describing difficulties remembering the names of people or places)
Signs and symptoms in Alzheimer’s Disease and Lewy Body Dementia?
Alzheimer’s Disease-
Sign: Hippocampal volume loss, impairment on memory tests
Symptom: Patient reports forgetting what spouse said
Lewy Body Dementia-
Sign: Impairment of visuospatial testing
Symptom: Well-formed visual hallucinations
Evidence of significant cognitive decline in one or more
cognitive domains based on:
1. Concern of the individual, a knowledgeable informant, or the clinician
2. A substantial impairment in cognitive performance,
preferably documented by standardized neuropsychological testing
The cognitive deficits interfere with capacity for independence in everyday activities.
_________________________ is the term used to describe the condition of individuals whose cognition lies between the cognitive changes of aging and early dementia.
Mild cognitive impairment (MCI)
They have objective evidence of cognitive impairment that represents a decline from the past, but they function independently or nearly so in their daily lives in a manner that is indistinguishable from the past.
Will everyone with MCI will develop dementia?
No, but if cognitive loss continues to worsen, may develop dementia
Evidence of a modest cognitive decline in one or more cognitive domains based on:
1. Concern of the individual, a knowledgeable informant, or the clinician
2. A modest impairment in cognitive performance,
preferably documented by standardized neuropsychological testing
The cognitive deficits do not interfere with capacity for
independence in everyday activities.
What is Cortical Dementia Syndrome?
Deficits arising from brain damage that primarily affects the cerebral cortex
What is Subcortical Dementia Syndrome?
Deficits arising from brain damage that primarily affects subcortical structures (e.g., basal ganglia, thalamus)
Name examples of Cortical Pathology.
Name examples of Subcortical Pathology.
Name examples of Mixed Pathology.
Cortical Pathology- Alzheimer’s Disease, Frontotemporal Dementia
Name examples of Subcortical Pathology- Parkinson’s Disease, Huntington’s Disease
Name examples of Mixed Pathology- Dementia with Lewy Bodies, Vascular Dementia
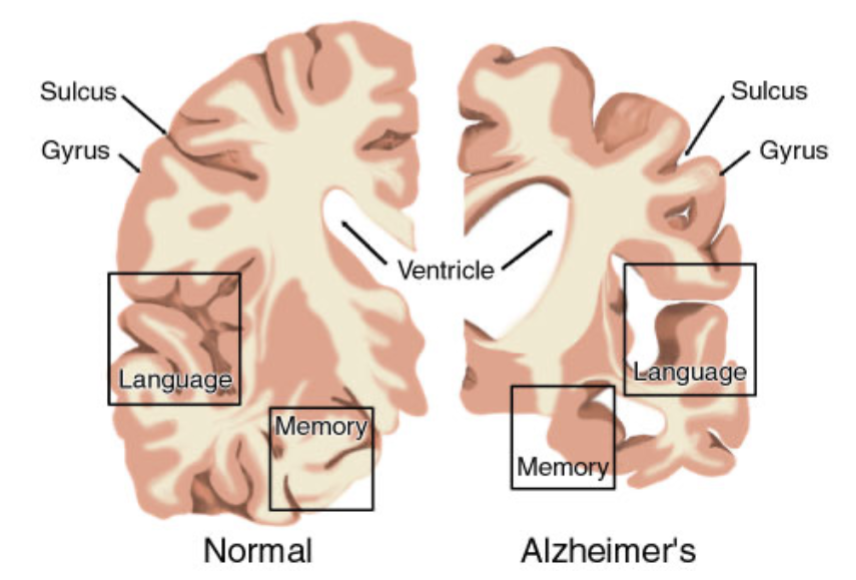
Indicators for Alzheimer’s Disease:
formation of amyloid plaques and tau tangles
cortical atrophy, neuron loss, and synapse loss
increased ventricles, decreased memory and language sections of brain
What is Early-Onset Alzheimer’s Disease (EOAD) and it’s deterministic genes?
occurs before age 65
accounts for 5-10% of all AD cases
PSEN1, PSEN2, APP virtually guarantee development of AD
What is Late-Onset Alzheimer’s Disease (LOAD) and it’s risk gene?
occurs after age 65
accounts for~90% of all AD cases
APOE increases risk for AD
What are the three allelic variants of the APOE gene? What are the combinations, meanings and prevalence?
e2- may provide protection against disease
e3- neutral role in disease
e4- increases risk for Alzheimer’s disease + associated w/ earlier disease onset
e3/e3 - 60%
e2/e4, e3/e4 - 20-30%
e4/e4- 2%
e2/e3, e2/e2- 10-20%
What the the signs of Alzheimer’s Disease?
Language production and comprehension
Prominent amnesia with rapid forgetting
Visuospatial impairments
Processing speed
Marked executive function
A significant deficit in episodic memory is usually the earliest and most prominent manifestation of Alzheimer’s disease.
What does APOE do?
It provides instructions for a protein called apolipoprotein E which affects the pathogenesis of AD through multiple biological pathways (Aβ aggregation and clearance)
What are the characteristics of early stage Alzheimer’s?
lasts ~2-4 years
Often not recognized by friends and family
Repeatedly asking questions or making
statements
Misplace items
Get lost easily
Word finding problems
Personality changes
What are the characteristics of moderate stage Alzheimer’s?
lasts ~2-10 years
Usually obvious to family and others
Wandering, pacing, disruptive behaviors
Delusions (often paranoid) and hallucinations
Require supervision
Sleep cycles disturbed
Sun-downing and radical mood swings
common
Require help with basic care activities
What are the characteristics of late/advanced stage Alzheimer’s?
• Lasts 1-3 years
• Little or no self care abilities
• Cannot speak or understand language
• Bedbound, chair bound, unable to walk
• Cannot recognize even closest relatives
• Difficulty swallowing, pneumonia is common
• Brain no longer can control body
What do symptomatic drugs do?
Symptomatic treatments address the cognitive & behavioral symptoms of AD (do not stop or prevent disease)
What do disease modifying drugs do?
Disease modifying agents affect the underlying pathophysiology (designed to preventing onset or progression of AD)
Define Parkinson’s Disease.
Progressive neurodegenerative disorder that affects balance and motor control regions of the brain (early/late around 50)
Characterized by loss of dopaminergic neurons in basal ganglia & substantia nigra. Main pathology is alpha synucleinopathy (Lewy Body).
What is the first symptom of Parkinson’s?
Resting tremor (starts on one side (L or R onset) then progresses to bilateral)
Which genes are linked to Parkinson’s? (15% familial)
LRRK2, PARK7, PINK1, PRKN, or SNCA
What abilities are associated with the Mesocortical, Nigrostriatal, and Mesolimbic areas of the brain, respectively? (Dopaminergic Pathways)
Mesocortical- cognition, memory, attention, emotional behavior, learning
Nigrostriatal- Movement & sensory stimuli
Mesolimbic- pleasure & reward seeking behaviors, addiction, emotion, perception
What are the hallmark behavioral features (motor symptoms) of Parkinson’s Disease?
Tremor, rigidity, postural instability, & bradykinesia
What are non-motor (non-movement) symptoms sometimes referred to as?
“invisible” symptoms (can’t be seen from outside)
autonomic system dysfunction-
constipation, low blood pressure, sexual dysfunction, urine incontinence
mood-
apathy, depression, visual hallucinations
physical-
drooling, dysphagia, fatigue/sleep problems, speech problems, masked facies
What the the cognitive sxs of Parkinson’s Disease?
microphagia
neuropsychiatric features: apathy, anxiety, depression
visuospatial impairments
marked executive dysfunction
dysphonia & dysphagia
memory profile: retrieval deficits
(relatively spared in early phases)
Categorize free recall, cued recall, recognition, and recognition discriminability for AD Encoding Deficit and PD Encoding Deficit, respectively?
. AD PD
Free Recall: Impaired> Impaired
Cued Recall: Impaired Improved
Recognition: Impaired Improved
Recognition
Discriminability: Impaired OK
What are some examples of treatments of Parkinson’s Disease? (symptomatic)
Pharmacotherapy-
dopaminergic drugs
Behavioral-
speech therapy
occupational therapy
physical therapy
exercise programs
Surgical-
deep brain stimulation
What are some of the stats on prevalence of vascular dementia?
30% of population will eventually have a stroke
→ 64% of those will develop cognitive impairment
→ 30% of those will have dementia
Overlap with AD (34% of all dementia have vascular pathology)
(inconsistent criteria & cognitive findings)
What are some characteristics of vascular dementia?
Infarcts + ischemic (loss of blood flow) strokes or hemorrhagic (burst of blood vessel) ruptures.
Due to single or multiple infarcts; small vessel disease
• White matter hyperintensities: reduced blood flow/degeneration of white matter
• Related to hypertension, other vascular risk factors
(e.g., diabetes, smoking)
• Associated with greater risk of stroke, cognitive impairment,
progressive cognitive decline
PROBLEM: How to quantify the location & size of infarcts in a way that is logically related to severity of cognitive impairment
What the the cognitive sxs of Vascular Dementia?
attention/processing speed impaired
more severe executive dysfunction
memory profile: retrieval deficits
executive dysfunction more severe than memory declines
When the term “healthy disparity” was coined in 1990, what was it meant to refer to?
It was specifically intended to denote worse health among socially disadvantaged people RATHER THAN all possible health differences among all possible groups of people
Distinguish between inequality, disparity, and inequity.
health inequality- differences in the health of individuals or groups (w/o moral judgment on whether observed differences are fair or just)
health inequity- (disparity) specific type of health inequality that denotes an unjust, avoidable difference in health
Why are there health disparities?
They are produced and sustained by deeply entrenched systems that intentionally and unintentionally silence.
These systems of power & structural drivers are not based on what is morally right or fair.
Distinguish between equality, equity, and justice.
equality- does not address the centuries of unequal treatment that have intentionally robbed entire communities of the vital resources needed to thrive.
equity- improves access to resources & create better conditions.
justice- fixes upstream drivers & systems.
Describe the Heckler Report
examined the health status of Americans by race/ethnicity and identified the gaps in disease rates, mortality, and other outcomes among Blacks compared to Whites
Black experienced ~60,000 excess deaths each year for people under 70
What six causes attributed to 80% of excess deaths in the Heckler Report?
heart disease and stroke
homicide and accidents
cancer
infant mortality
cirrhosis
diabetes
Is race biological?
No. Our species does not have enough genetic variability among its populations to justify either the identification of geographically based races or evolutionarily distinct.
Race is socially constructed. l.ineages
What is ethnicity?
a socially constructed way of grouping that emphasizes cultural commonalities (e.g., national origin, language, religion, geography and/or family origin)
What is the largest minority group in the US?
Hispanic/Latinos]
Spanish-speaking countries, or have ancestral ties to Spain or Latin American
People of Latino/a/x or Hispanic backgrounds can be of any race (e.g., Black, white, Indigenous/Native American Asian, or identify with multiple more races)
What is every US Census Racial Category?
• White – A person having origins in any of the original peoples of Europe.
• MENA - Middle East, or North Africa (not usually classed properly because under “White” most of time… part of issue with census
• Black or African American – A person having origins in any of the Black racial groups of Africa.
• American Indian or Alaska Native – A person having origins in any of the original
peoples of North and South America (including Central America) and who maintains
tribal affiliation or community attachment.
• Asian – A person having origins in any of the original peoples of the Far East, Southeast Asia, or the Indian subcontinent including, for example, Cambodia, China, India, Japan, Korea, Malaysia, Pakistan, the Philippine Islands, Thailand, and Vietnam.
• Native Hawaiian or Other Pacific Islander – A person having origins in any of the
original peoples of Hawaii, Guam, Samoa, or other Pacific Islands.
• Some Other Race - for people who do not identify with any of the other race categories.
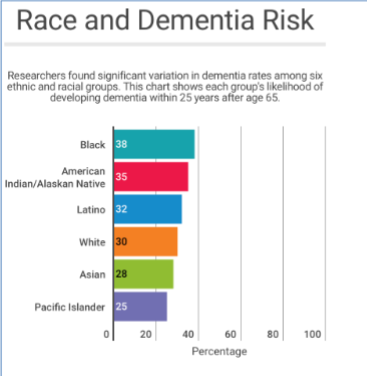
Which racial/ethnic group has the highest rate of dementia?
African Americans > American Indian > Latino
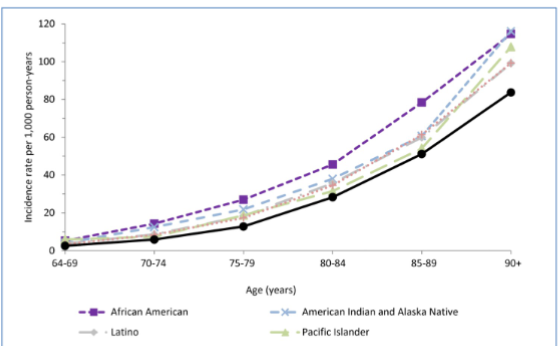
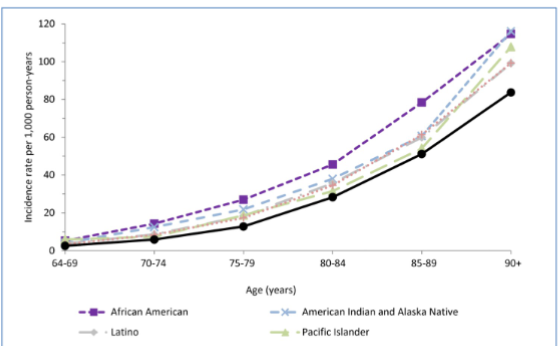
What is the difference between dementia prevalence & incidence?
prevalence- number of cases of dementia in a population at a particular time point
incidence- number of new cases in a population over a period of time
Which racial/ethnic groups experiences drastic increases in dementia incident in old age (90+)?
Pacific Islander + Asian American
What do you make of the Asian American estimates regarding racial/ethnic disparities in AD?
Asian American estimates are underrepresented.
Only 18% of Asian Americans are aware of MCI. This can make it harder for
individuals or families to recognize the symptoms and seek professional care.
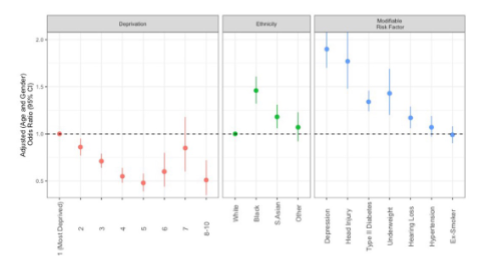
Based on the UK sample we looked at, which ethnic group is at increased risk for dementia?
South Asian (still highly heterogenous sample, so more research needed)
What is the paradoxical trend regarding Alzheimer's Disease (AD) in African Americans and Hispanics compared to Whites?
Although the rate of AD in African Americans and Hispanics is higher than in Whites, they are less likely than Whites to have a diagnosis of the condition.
What is a consequence of African Americans & Hispanics being typically diagnosed in later stages of Alzheimer’s?
more cognitively and physically impaired—& therefore in need of more medical care ($$$!)
Why are Black and Hispanic/Latino older adults less likely to be diagnosed with AD?
• Less likely to present for care
• Less likely to have have access to early/critical care initiatives
• Clinicians may have a harder time diagnosing earlier stages of MCI/dementia
• Neuropsychological measures are culturally biased (more on this soon)
• Clinicians are not adequately trained or prepared to consider relevant cultural factors of influence
• Perceptions of care & historical injustices
• Discrimination
Why haven’t they been included in AD clinical trials?
not aware of clinical trials
distrust of medical/scientific community
Describe a common timeline of AD diagnosis for a disadvantaged racial minority.
initial assessment, diagnosis and referral
delayed diagnosis
misdiagnosis
fewer specialist referrals
ongoing treatment and support
less likely to receive & more likely to discontinue antidementia meds
increased antipsychotic use
increased hospital mortality
higher cost of health care
later stages, end of life care
reside in nursing homes with lower quality of care
less advanced care planning
more aggressive and costly care
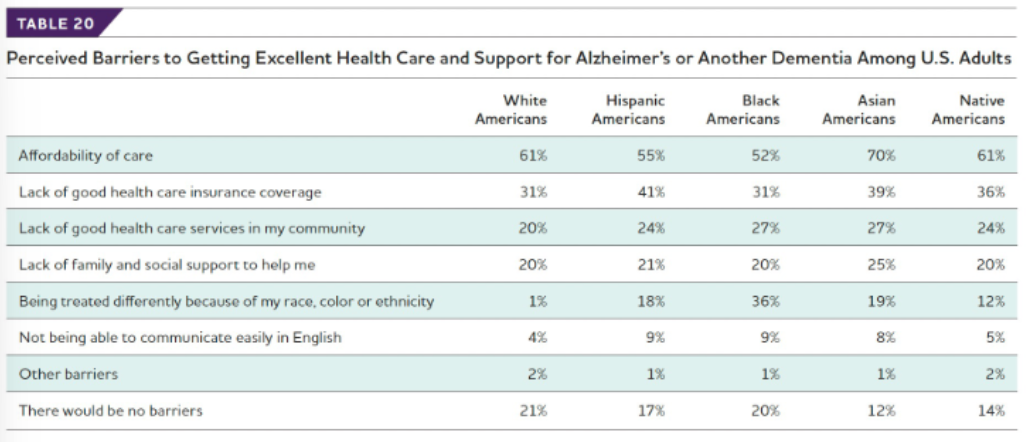
What are the two biggest perceived barriers to care for all racial/ethnic groups?
affordability
lack of good health care insurance coverage
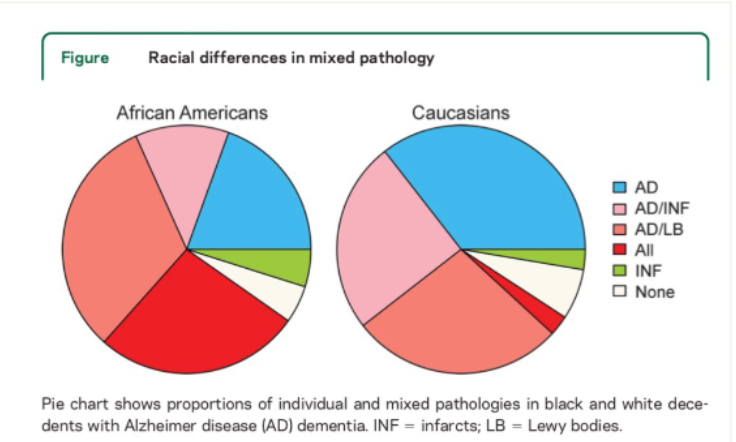
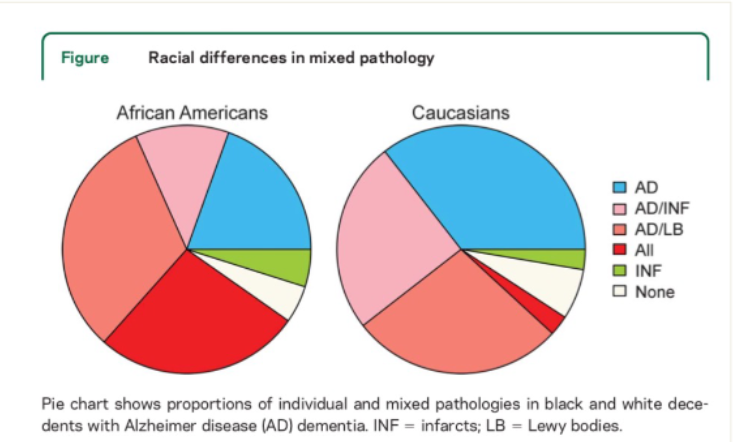
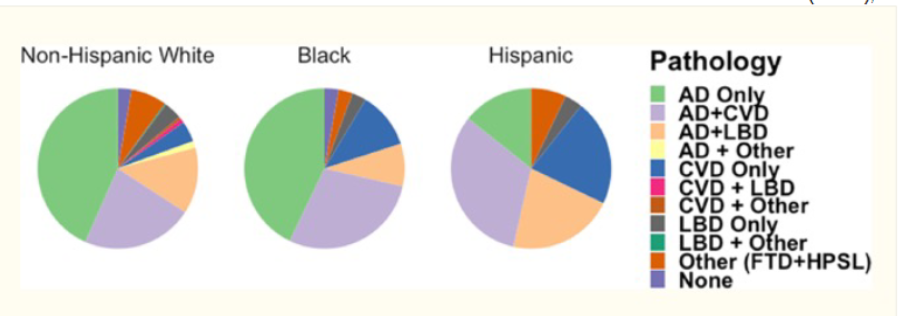
What can we say about the underlying pathology for racial/ethnic minorities at increased risk for AD?
It looks different from White people. Rates of cardiovascular disease are higher (clearly plays role in AD manifestation)
Which group has a greater proportion of pure AD pathology?
Caucasians
Which group has a greater proportion of All types of pathology?
African Americans
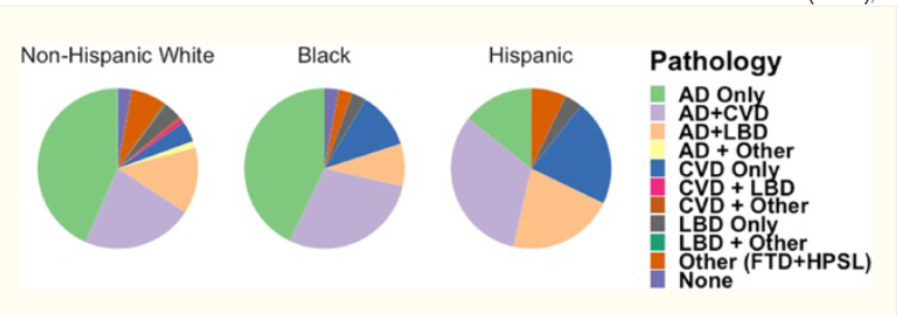
Which group has the smallest proportion of pure AD pathology?
Hispanic
Which groups have a greater proportion of CVD and AD+CVD pathology?
Hispanic, then Black
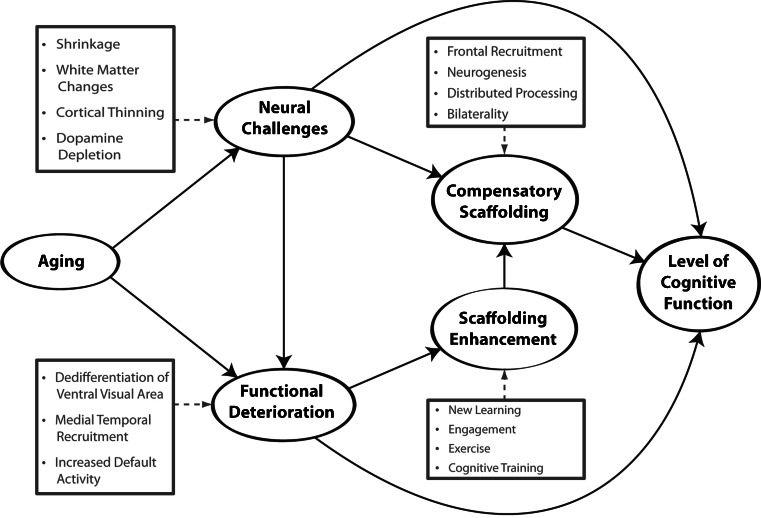
What can we say about the neuroimaging metrics for racial/ethnic minorities at increased risk for AD?
It looks different. Minority groups more likely to be exposed to
neural resource depletion factors (remember STAC-r model)
Cumulative social disadvantage is a key factor in AD disparities.
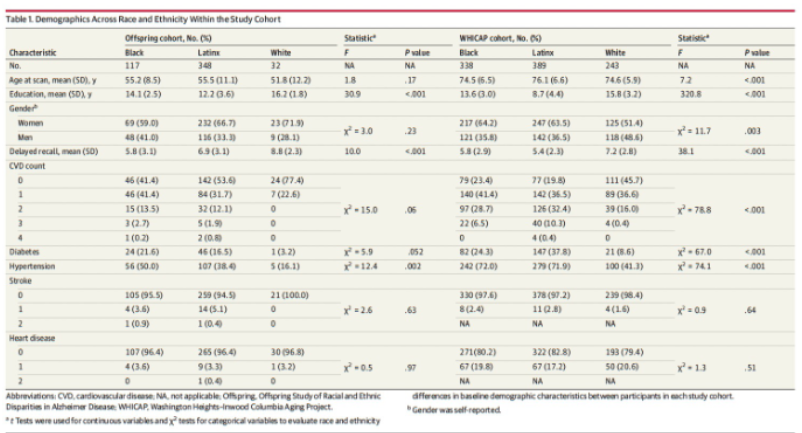
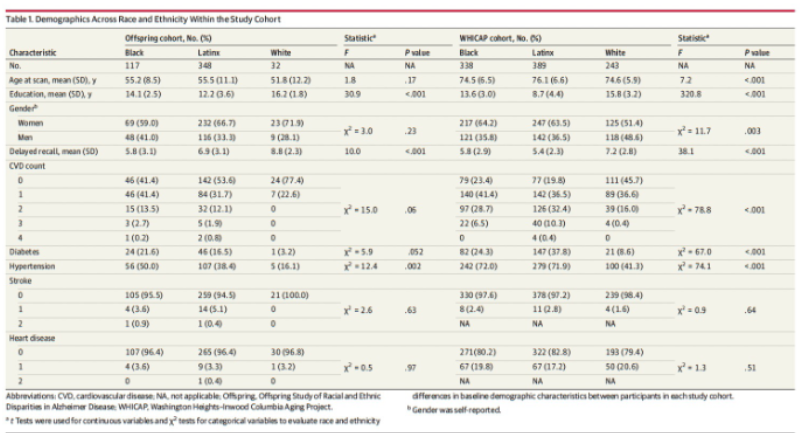
Where are there significant differences in brain metrics between the racial groups?
in the WHCAP group (older generation)
Are these patterns different across cross-generational cohorts?
Context between parent and offspring are different. Disparities increase over time in terms of cortical thickness and white matter volume… because parent generation is older and that’s when AD pathology starts appearing
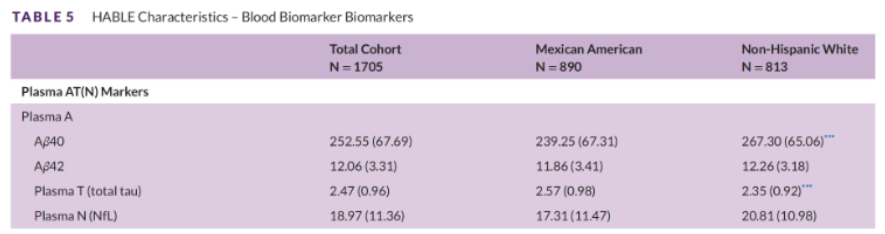
In a large scale Texas study, which group showed higher levels of amyloid, Whites or Mexican Americans? What about tau?
Whites showed higher levels of amyloid. Mexicans showed higher levels of tau.
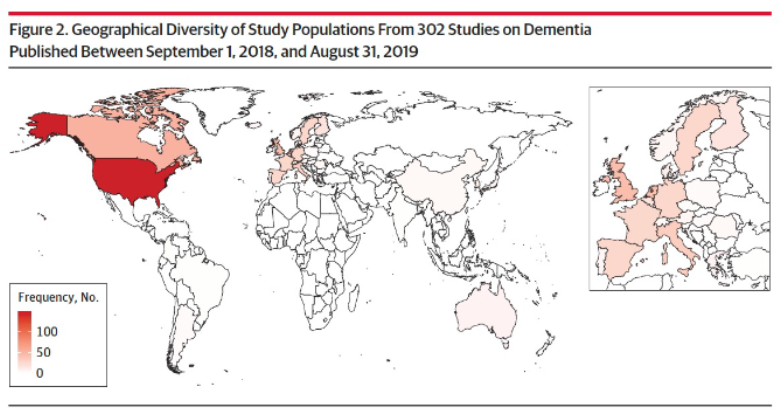
What is the WEIRD problem in science?
W: Western
E: Educated
I: Industrialized
R: Rich
D: Democratic
The reliance on homogenous convenience samples in science has hindered our explorations of understanding dementia risk in diverse groups.
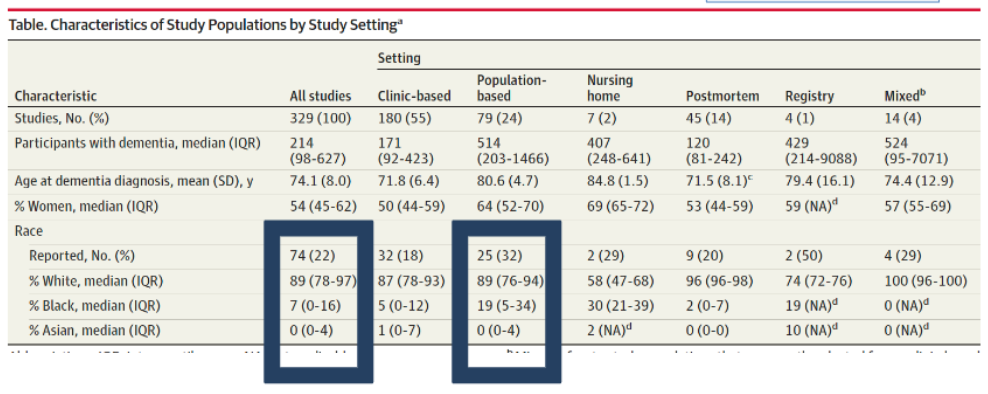
What settings do we see Blacks underrepresented in AD studies?
in post-mortem and clinic-based studies
Sex assigned at birth
sex assignment by doctors that is usually based on genitals (e.g., male or female)
Gender identity
internal experience and understanding of our own gender
Gender Expression
the way in which we present ourselves, which can include physical appearance, clothing, or behaviors
Sexual orientation
different forms of attraction; can be attracted to one gender, multiple genders, or different genders throughout your life
Sexual Minority
encompasses lesbian, gay, two-spirited, bisexual, and queer identifying populations
Gender Minority
umbrella term for transgender & non-binary people whose gender identity/expression does not conform to social expectations based on their sex assigned at birth