





peds GI
Formula Intolerance
Signs of formula intolerance:
Diarrhea, vomiting
Blood or mucus in stool
Pulls legs up towards abdomen in pain
Difficulty gaining weight
Switching formulas should stop issues
Milk protein allergy: can cause vomiting, blood in stools, hives, irritability, wheezing, cough, congestion, reflux
Must use hydrolyzed formulas
Can do stool sample to test
If breastfeeding, mother must avoid all milk products & soy
Gastrointestinal Reflux
Occurs when gastric contents reflux back up into esophagus, making esophageal mucosa vulnerable to injury from gastric acid
Smaller stomach, shorter esophagus, and immature esophageal sphincter muscle = contributes to increased symptoms in infants
GERD = tissue damage from GER
Risk factors: prematurity, neurological impairments, asthma, Cystic Fibrosis, cerebral palsy
Peak incidence occurs at 4 months old
About 40% of infants experience GER
Must differentiate between GERD / GER
Expected findings:
Infants: spitting up or forceful vomiting, irritability, excessive crying, blood in vomit, arching of back, stiffening – colicky baby
Failure to thrive
Apnea (ALTE/BRUE) or other Respiratory problems (choking with feedings, cough)
Children: heartburn, abdominal pain, difficulty swallowing, chronic cough, noncardiac chest pain
If inflammation left untreated, scarring and strictures may form
Management of GER
None: if gaining weight & happy
Nursing Care:
Small, frequent meals
Avoidance of foods that worsen reflux
Elevate head after meals
Avoid foods that worsen reflux: caffeine, citrus, peppermint, spicy or fried foods
Medication
PPI: omeprazole (Prilosec), lansoprazole (prevacid)
Most effective when given 30 mins before breakfast
Need to take for several days before improvement
H2 receptor antagonists (cimetidine, ranitidine (zantact), famotidine (Pepcid)
Helps to reduce gastric secretions, may stimulate some increase in esophageal sphincter tone
Thickened feedings (usually rice cereal or oat cereal)
Feeding tubes: if unable to gain weight
If aspiration risk: will need duodenal or jejunal feeding tube (G or J tube) or surgery (Nissen Fundoplication)
Nissen Fundoplication
Operation done to tighten the outlet of the esophagus as it empties into the stomach
Wraps fundus of stomach around the distal esophagus
Necessary for children who have complications related to aspiration or for those who have persistent symptoms that are not relieved by medication
Appropriate for patients with loss of tone over time
With or without G-tube
Diet after surgery should start slow with clears, then soft foods
Acute Gastroenteritis
An inflammation of the stomach and intestines
Most common causes: viruses, bacteria (food poisoning), and intestinal parasites
Viruses: usually cause of mild gastro; Norwalk-like virus (norovirus), adenoviruses, enterovirus and rotaviruses
Bacteria: usually produce high fevers, severe GI symptoms, and dehydration; campylobacter, salmonella, E. Coli (sicker, more severe), watch out for dehydration
Parasites: Giardia lamblia
Presentation: vomiting, diarrhea, generalized abdominal pain, fever
Education:
Decrease spread (make sure to wash hands, especially after diaper changes wash toys)
Maintain hydration, small amounts more frequently
Watch for signs of dehydration
Treatment depends on cause
Virus: self-limiting,, comfort care
Bacteria: antibiotic depending on cause
Parasite: Giardia treat with metronidazole (Flagyl)
Dehydration
Levels:
Mild: behavior, mucous membranes, anterior fontanel, pulse, and blood pressure within expected findings
Possible slight thirst
Moderate: pulse slightly increased, dry mucous membranes, decreased tears, normal to sunken anterior fontanel on infants
Cap refill 2-4 seconds
Possible thirst and irritability
Severe: tachycardia present, orthostatic blood pressure can progress to shock, dry mucous membranes, no tearing, sunken eyeballs, sunken anterior fontanel
Cap refill > 4 seconds
Oliguria or anuria
Nursing actions:
Oral rehydration FIRST for mild-moderate dehydration
If unable to drink enough to correct fluid losses, will need IV
Assess cap refill, monitor vital signs, monitor weight, maintain accurate I&O
start with pedialyte for young children and gatorade in older children
give 10-15 mLs every 15 minutes
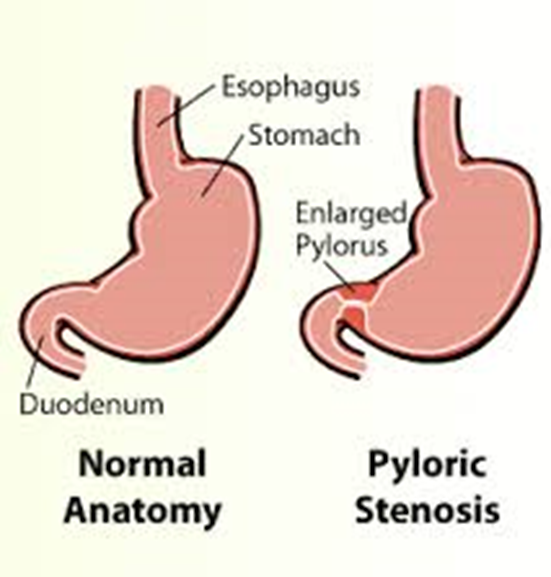
Pyloric Stenosis
Pyloric sphincter= ring of smooth muscle between the stomach and the duodenum
Thickened pyloric sphincter creates narrowing & obstruction
As stomach continues to try to push food through, peristalsis becomes so powerful that food is ejected into the esophagus and out of the mouth = projectile vomiting
More common in first born males
Most common at age 3 weeks
What does it look like:
Failed formula changes
Projectile vomiting
Dehydrated
Constant hunger
Fluid electrolyte imbalance
Risk for metabolic alkalosis
On exam, olive shaped mass in RUQ
constant hunger because milk is not making its way through
hyperkalemia
metabolic alkalosis because of all the vomiting
pyloric sphincter is so hard
Management of Pyloric Stenosis
Need an ultrasound to confirm
Need to correct fluid and electrolyte imbalance
*at risk for hypokalemia & metabolic alkalosis*
Need surgery
Nursing Considerations:
Need fluid support prior to surgery
NPO prior to surgery
4-6 hours postop can start clear liquids like pedialyte
24 hours can go to formula or breastmilk
Pain management
Slow feeding protocol after surgery
Anticipatory guidance about setbacks
Hirschsprung’s Disease
Aka Congenital aganglionic megacolon
Stools have ribbon pattern
Congenital condition in which the nerve cells of the myenteric plexus are absent in the distal bowel & rectum
Is a sustained sympathetic stimulation (cannot relax)
Decreased enteric nerve stimulation (loses motility)
Results in decreased motility & mechanical obstruction
Rectal internal sphincter cannot relax
Absence of parasympathetic ganglion cells in end of large intestine near rectum
Diagnosis:
rectal biopsy to confirm absence of ganglion cells
X-ray: with contrast, will see dilated portions of colon
Risk Factors: male gender, genetics, trisomy 21
Hirschsprung’s Infant presentation
will not pass meconium
will see vomiting,
can either be bile stained or of fecal material
will see abdominal distension, constipation
anorexia and poor feeding
may see temporary relief with enema
Hirschsprung’s Older Children presentation
History of constipation since birth
Distension of abdomen
Thin abdominal wall with observable peristaltic movement
Stool appears ribbon like, fluid like, or in pellet form
Failure to grow; will see loss of subcutaneous fat
Child may appear malnourished or have stunted growth
Anemia
SARCASM
Sigmoid colon
Absence of movement
Ribbon shaped stool & Rectal biopsy for diagnosis
Congenital / will see constipation
Abdominal obstruction / abnormal feeding
Syndrome (common in those with Down Syndrome)
Meconium (infant will not pass in first 24 hours)
Management
Surgery to remove aganglionic bowel
“pull through” normal section pulled through colon and attached to anus
If very ill, surgery will be done in two steps; will have temporary ostomy while gut heals
High protein, high calorie, low fiber diet
May need TPN in some cases
Monitor for signs of enterocolitis
Complication
Hirschsprung’s associated enterocolitis = inflammation and obstruction of intestines
Occurs in about 20% of neonates with Hirschsprung
Perforation of obstructed bowel
Presenting symptoms:
Foul smelling diarrhea either with or without blood
Fevers
Abdominal distension
Lethargy
Poor feeding
LIFE THREATENING – can lead to toxic megacolon and perforation of bowel
Can lead to sepsis if not treated urgently
Need antibiotics, fluid resuscitation, and decompression of obstructed bowel
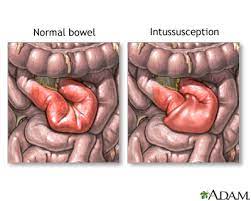
Intussusception
Telescoping of bowel on itself
Results in lymphatic and venous obstruction leading to edema
With progression/ no treatment, ischemia and increased mucus into
intestine will occur
Most common in those 3 months to 6 years
More concerning if patient older
Findings:
Sudden, excruciating pain (drawing knees up to chest)
Currant jelly stools
Palpable abdominal mass (sausage shaped)
May see vomiting, fever, distended abdomen
Treatment:
Air enema
surgery
most common in infants under 1 but can happen in up to 6
first symptoms: abdominal screaming, pulling knees up to chest
slough of mucus and blood - jelly stool
can be fever if infection, ischemia,
air enema - pressure from air will untelescope intestines - has to be done in radiology - we watch for signs and bowel perforation
can try air enema again but if that doesn't work will go to surgery
because of ischemia possibility will do air enema pretty quickly after confirmed diagnosis
The extreme: Short Bowel Syndrome
Aka “short gut”
Loss of so much bowel, can’t be nourished enterally
NEC
Intussusception
Hirschsprung
Gastroschisis
Will be TPN dependent
Will need central line
Liver burden
Failure to Thrive
Often have severe diarrhea due to accelerated intestinal transit, gastric acid hypersecretion, intestinal bacterial overgrowth, malabsorption of fats
can be due to condition or nonfunctional
cannot be fed enterally because not enough length in bowel to absorb
liver burden with TPN and lipids
Watch for signs of dehydration & electrolyte imbalances
May see diarrhea, greasy, foul-smelling stools
Fatigue
Weight loss
Malnutrition (can’t absorb everything because it moves through GI tract so rapidly)
Must monitor intake & output and weight
Complications:
Central line infections & sepsis
Chronic renal failure
Biliary Atresia
Complete or partial obstruction of the bile ducts inside or outside the liver
Congenital condition, ducts do not develop normally
Bile flow from liver to gallbladder is blocked 🡪 liver damage 🡪 cirrhosis of liver
Bile can’t flow so it backs up into the liver
Early diagnosis = key to prevent or slow liver damage
Will see increased AST, ALT, bili
scan (hepatobiliary iminodiacetic acid scan) to see if bile ducts / gallbladder are working properly; liver biopsy
Kasai procedure = only effective treatment
Removes biliary tree and adds new to drain bile
Hidascan to see flow of bili
Need liver transplant
Initially asymptomatic, then start with jaundice; as bili continues to rise will se distension and hepatomegaly
Presentation:
jaundice at 3-4 weeks
Distended abdomen
Dark urine (due to increased bili)
Pale or clay colored stools (due to bile pigments)
Slow or no weight gain
Bruising, bleeding, intense itching as it progresses
Failure to thrive is common
Constipation
A SYMPTOM NOT A DISEASE
A decrease in bowel movement frequency or increase in stool hardness for at least 2 weeks
Often associated with painful bowel movements, blood streaked or retained stool, abdominal pain, lack of appetite or stool incontinence
Trouble for more than 2 weeks
A triangle of frequency, consistency, ease
Frequency alone is not criterion
Caused by:
Structural causes:
hirschsprung's or other strictures
Systemic causes:
hypothyroidism, chronic lead poisoning,
can be side effect of medications: antiepileptic, opioids, iron
can be in kids just starting school because they don’t want to go or are scared to go
can lead to encopresis: leakage of stool around hard stool
*need to evaluate condition further if patient develops vomiting, abdominal distension, pain or evidence of growth failure; need to make sure there is nothing else going on
Treatment
Need to both restore normal bowel function & stooling pattern
First line: miralax
Osmotic laxative – draws water into stool
Usually takes 1-2 days for effect
Can cause incontinence, abdominal pain, nausea, bloating
Can also use:
Docusate sodium (senna): stimulant – acts as a local irritant in the colon, stimulating peristalsis
Can cause diaper rash, do not use in those <1 year old
Magnesium hydroxide: laxative – causes osmotic gradient leading to laxative effect (aggressive)
Diarrhea
Abnormal transport of fluid and electrolytes across intestinal mucosa
A sudden increase in frequency and change in consistency of stool
Major cause of illness under age 5
Can be mild to severe, acute or chronic
Chronic if more than 14 days
Causes
Viral, bacterial, parasitic
Associated with other infections such as URI, UTI
Dietary
Medicine-related
Viral diarrhea:
Most common cause of diarrhea in children <5 y/o
Fever
Onset of watery stools
Diarrhea for 5-7 days, vomiting for about 2 days
Transmission = fecal oral
Example: Rotavirus
Parasitic diarrhea:
Enterobius Vermicularis
Perianal itching, sleeplessness, restless
Ingested or inhaled eggs hatch in upper intestines and mature then migrate out of intestine & lay eggs
Giardia lamblia
Children < 5 = Diarrhea, vomiting, anorexia
Older children: abdominal cramps, malodorous, pale, greasy stools
Transmitted person to person, food or animals
Bacterial diarrhea:
Length of symptoms depends on source
Can be transmitted through undercooked meats, person to person, from pets, contaminated water
Examples: Yersinia, e. coli, salmonella, clostridium difficile, clostridium botulinum, shigella, norovirus, staph
More severe, higher fevers, worse symptoms
Nursing care for diarrhea
Obtain child’s weight at same time each day
Avoid rectal temps
Initiate IV fluids as ordered if needed
Administer antibiotics as prescribed (for Shigella, C. Diff, G. lamblia)
Avoid antibiotics with Salmonella and E. Coli
Avoid antimotility agents with E. Coli, Salmonella, Shigella
Education:
Child should stay home from school/ daycare during incubation period
Diet changes needed
Avoid fruit juices, stick to BRAT diet
Frequent skin care to avoid skin breakdown
Avoid antimotility agents because we want them to poop it out
To prevent spread of infection:
Clean toys and child care areas thoroughly
Hand hygiene after toileting and after changing diapers
Appendicitis
Inflammation of the vermiform appendix caused from an obstruction of the lumen of the appendix
Causes of obstruction: fecalith, stenosis, parasitic infection, tumor
Mucus continues to be secreted and bacteria grows causing increased pressure
impaired perfusion
Average age of presentation=10 years old
If untreated, can become gangrenous & ruptures
Rupture can occur within first 48 hours of complaint
More likely to rupture in younger children when not suspected
Can lead to sepsis and shock
Chief Complaint:
Vague midline pain that moves to RLQ and intensifies
Vomiting, diarrhea
Fevers
anorexia
Exam findings:
Rebound tenderness
Rigid abdomen
Guarding
Rovsing: palpation on the left lower quadrant of the abdomen results in pain in the right lower quadrant (at McBurney’s point)
Obturator: pain during internal rotation of right hip
Psoas: pain at extension of right hip
Enemas, heat packs, and laxatives can’t be given
Morphine, toradol, antibiotics: most common treatment/plan
Diagnostics:
Labs:
Electrolytes
Increased WBC
Urine
Imaging:
US versus CT
ultrasound first to avoid CT
can look for swelling
cannot be officially diagnosed without CT
Shift to left: increase in WBC
Nursing care pre and post appendectomy
Pre Appy
Monitor for signs of sepsis including increased heart rate and respiratory rate, fever, decreased bp
Watch for sudden relief of pain
Pain relief
Promote comfort
Administer antibiotics
NPO
Post Appy
Pain management
Semi-fowlers
Wound care (can either be laparoscopic or open)
NG tube for decompression
IV antibiotics
Prevention of complications
Wound infection
Line infection
UTI
Abscess
Pneumonia
Get up first day to get everything moving
Appendectomy complication
peritonitis (inflammation in the peritoneal cavity)
Signs: fever, sudden relief of pain after perforation followed by diffuse increase in pain, irritability, rigid abdomen, pallor
Failure to thrive
Weight for age that is less than the 5th percentile on multiple occasions or weight deceleration
Clinical Manifestations:
Poor weight gain
Vomiting, food refusal, food fixation
Irritability
Nonorganic causes: food restriction, food rituals, poor appetite
organic causes: vomiting, diarrhea
Diagnostics:
Height, weight, BMI
Feeding assessment (quality of food, ability to chew / swallow, 24 hour diet recall)
BMP, vit d, lead, zinc, iron
Albumin (with severe FTT)
CBC, ESR, electrolytes
Stool studies
Sweat chloride test
TSH
Celiac Disease
Gluten sensitive enteropathy
An autoimmune reaction to gluten that leads to intestinal inflammation, atrophy, and malabsorption
Gluten= protein found in wheat, rye, barley
Chronic, irreversible disease
In early onset, fat absorption is impaired, leading to excretion of large amounts of fat in the stool
As it progresses, there is a malabsorption of proteins, carbs, and fat-soluble vitamins
Diagnosis: transglutaminase IgA – if positive a biopsy of small intestine is done to evaluate intestinal mucosa damage
Should also get CBC, ferritin levels, iron levels – at risk for iron deficiency anemia
official diagnosis: get piece of intestine via colonoscopy
can do bloodwork to see if colonoscopy is necessary - but very expensive
Assessment findings:
Weight loss
Diarrhea
Vomiting
Foul-smelling stools
Delayed growth and development
Can get dermatitis herpetiformis (blistering, pruritic skin rash on elbows, knees, buttocks
Severe form:
Iron deficiency anemia
Vit b 12 deficiency
Osteopenia / osteoporosis r/t calcium malabsorption