
History of Health Care In Canada
Define:
Canadian Health Act: It Became law in 1984 under Pierre Trudeau. It provides equal, prepaid, and accessible health care to all Canadians. It must be managed by a public authority and a nonprofit.
Public Administration: The implementation of public policy
Comprehensive Coverage: All Canadians with a medical need have access to prepaid, medically necessary services provided by a doctor or hospital.
Universality: All residents of the province are entitled to uniform terms and conditions where the provinces can individually charge insurance premiums subsidization is required.
Portability: If leaving your province, you are still entitled to free health care for up to 6 months (except Ontario which is 212 days (about 7 months) of any given year)
Accessibility: Citizens are given reasonable access to where and when needed and paid for by the government
Medically necessary: A clinical judgment made by the attending physician to determine the necessity of a medical procedure or service
User charges/ fees: Under the Canada Health Act this is not allowed If the province does not cover the service the federal government will
Catastrophic drug costs: Government gives more money to those with higher drug plans
Reasonable access: Access to services when and where they are available
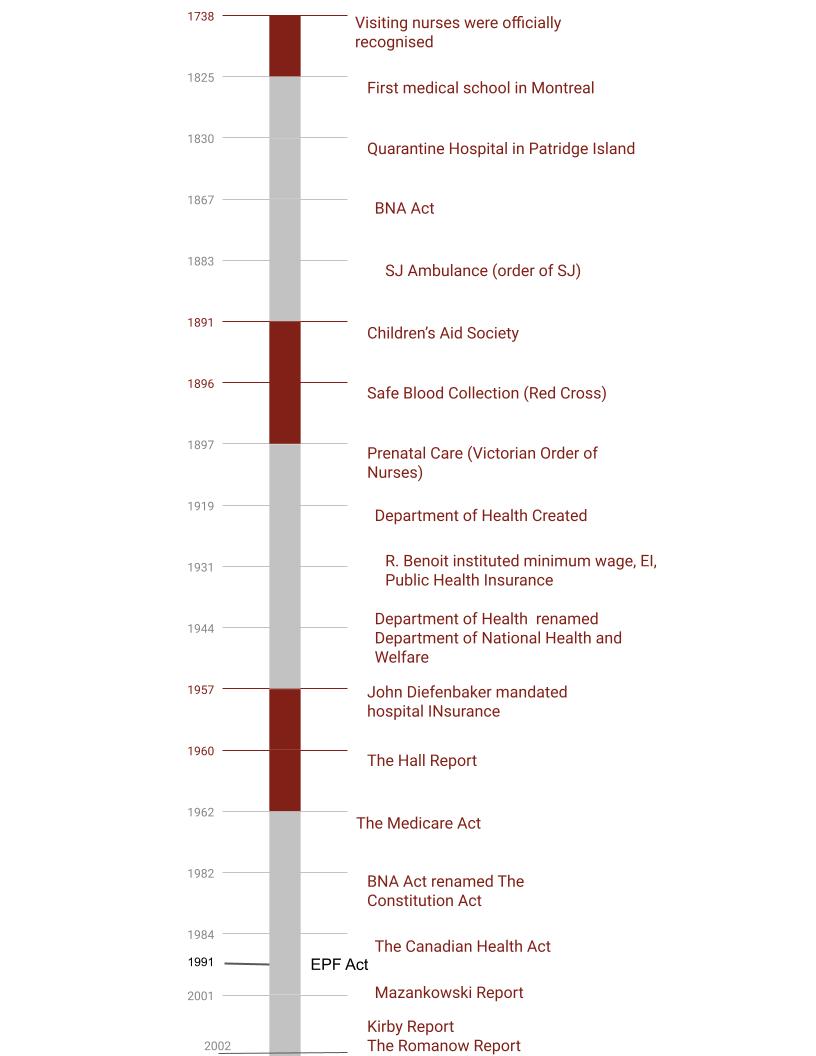
Evolution of Health Care
1500's/1600s settlers came down and started to create spots for doctors' nurses etc. All was governed by charitable organizations/ the church (catholic)
If a doctor was needed you would have to pay for one to come to your house
Ontario and Quebec established boards of health in 1832 and 1833
These boards were designed to:
Enforce quarantine and sanitization laws
Impose restrictions on immigration (disease spread)
Stop the sale of spoiled food
John Diefenbaker in 1957 introduced Hospital Insurance which provided federal dollars to provinces and territories to create a hospital insurance plan
It funded half the price of hospital bills
Allied health in a hospital setting
Outpatient clinics
Legislation Leading up to the Canada Health Act
The Hall Report: 1960 called for a national health insurance program. Also, recommend that we need more doctors and hospitals.
The Medicare act: 1966 Ottawa would pay half provinces would pay the other half
The Established Program Financing Act: 1977 50/50 arrangement fell through, and the government started to block payments every 2 months
EPF Act: doctors were capped on how much they could make
1984 The Canada Health Act became law under Pierre Trudeau
Information: the federal government has access to all citizen’s files
Recognition: public recognition the federal government pays for said services
Extended health services considered medically necessary in the Act included:
Intermediate nursing home care
Adult residential care services
Home care services
Services provided in an ambulatory care center
Uninsured services include:
Private hospital rooms
Private nursing duties
Telephone/television
Prescription over the phone
Medical certificate for work school, insurance, etc.
Cosmetic services
The Three major reports
The Mazankowski Report: A framework for reform (2001)
Purpose to preserve healthcare services for Alberta
By letting doctors perform privately after x number of years
Making elective services out of pocket
Creating province-wide records and health Cards
Alberta pays too high taxes
2003 Alberta has province-wide records and health cards
The Kirby Report: The Health of Canadians- Federal Role 2002
Purpose: Canadian Health Care system pertaining to the Federal Government
Like the Mazankowski Report
Unsustainable to be left alone
Taxes gauged on income
Creating wait times; then shipping patients elsewhere to receive treatment (reasonable Access) all paid for by the government
Government funding for medications depends on income
$4.5 billion to go towards information technology and advanced medical equipment
Government incentive to come and work in Canadian healthcare
Ontario adopted taxes gaged on income
The Romanow Report: Building on Values: The Future of Health Care in Canada (2002)
Purpose: Adapt Canada’s Health Care System, create disease prevention and awareness to promote health
Like the Mazankowski Report
Got Canadians’ opinions through forums and meetings held across the country
The belief that Universal health care was sustainable but needed to figure out how (readjusting)
Opposed private healthcare
Create a council to improve health care, maintain the system, and report to the citizens
Accountability to the Canadian Health Act
Coverage for homecare, diagnostic testing, palliative care, and mental health care
EI and job security to extending family for taking care of loved ones
Drug costs are subject to the terms and conditions covered
New drugs should be monitored and tested federally; drug prices are kept in a range
Wait times be monitored but not limited
(2004) $10 billion dollars will be put into health care over ten years
(2004) Council was created and funds health care, postsecondary education, and welfare
Wait times have been limited and monitored
Funding for information and technology as well as EI/job security
Drug prices have been monitored in most provinces and tested federally
Review Questions
What were the health care responsibilities of the federal and provincial governments outlined in the British North America Act?
What organizations attended to the healthcare needs of Canadians in the eighteenth and nineteenth centuries?
What are three traditional healing practices of Canada's Indigenous population? Briefly describe them.
How and when was health insurance first introduced in Canada?
How and when was the concept of prepaid hospital care introduced in Canada?
List and describe three pieces of legislation that played significant roles leading up to the creation of the Canada Health Act.
What are the criteria and conditions of the Canada Health Act and what do they mean?
8. What is meant by the terms medically necessary, extra billing, and user charges, and how do
they relate to each other in the context of the Canada Health Act?
9. What are the goals of primary care reform? (p.27)
10. Why was the Indigenous population in Canada so affected by disease when non
Indigenous people came to Canada?
11. Describe two healing ceremonies important to First Nations people in Canada. Which ones are practiced today?
12. How did residential schools affect the Indigenous population in Canada?
Review Answers
Establishing and maintaining marine hospitals, caring for the indigenous people, and management of quarantine.
Charitable and religious organizations (Catholic mostly) including the nursing sister from 1639-1867.
Sweat lodge- a person deprives themself of food for up to 4 days to weaken the physical self, making them venerable and more receptive to advise and teaching of the spiritual world
Willow tree bark for headaches
Dandelions to help with rashes, boils, and inflammation
Gooseberries to help with constipation
1966 The Hall Report stated national Medicare and fully implemented in 1968
1957 John Diefenbaker introduced it. The Hospital Insurance and Diagnostic The Services Act states it is obtained without having to pay out of pocket since it is paid for by the federal government.
Hall Report- called for nation health insurance and said we need more doctors and hospitals
Medicare Act- says Ottawa will pay half and the individual provinces will pay the rest.
EPF Act- Government will make block payments every 2 months based on how much the provinces gave out. Doctors were also capped on how much they could make.
-Public Administration: managed by a public authority on a nonprofit basis. The answer to the government is overseen by the Ministry of Health.
-Information: the federal government has access to all citizen’s files
-Comprehensive Coverage: All Canadians with a medical need to access prepaid, medically necessary services provided by a doctor or hospital.
-Recognition: public recognition the federal government pays for said services
-Universality: All residents of the province are entitled to uniform terms and conditions where the provinces can individually charge insurance premiums subsidization is required.
-Portability: If leaving your province, you are still entitled to free health care for up to 6 months (except Ontario which is 212 day (about 7 months) of any given year)
-Accessibility: Citizens are given reasonable access and paid for by the government
Medically Necessary is a term where the doctor states whether the patient is covered or not.
Extra Billing -doctors charged patients out of pocket on top of the government funded prices
User charges are a fee charged to a patient for a service that
should be supplied under the Act; however, the province or territory does not cover itCollaborative, Team-oriented, Community-based care
Disease prevention
More holistic approaches
The indigenous have not been around the diseases so their immune system did not help them. They lacked natural cures since the diseases were not originally from there.
An Eagles feather has been brought into the RCMP as a sort to swear an oath upon.
Medicine Wheel- a person acknowledges their physical cognitive emotional and spiritual self and accepts responsibility to regain full health.
They negatively impacted them, forcing the children out of their homes to be assimilated and dead leaving them with multi-million dollars to help cope.