Looks like no one added any tags here yet for you.
OBJECTIVE: List the infecting pathogens in community-acquired bacterial meningitis
*streptococcus pneumoniae 2+ years
group b streptococcus (streptococcus agalactiae) *babies
neisseria meningitidis *2+ years
haemophilus influenzae type B *2+ years
listeria monocytogenes *50+ years
OBJECTIVE: List the infecting pathogens in healthcare-associated meningitis and ventriculitis
CSF shunts
CSF drains
intrathecal infusion pumps
deep brain stimulation hardware
neurosurgery
head trauma
OBJECTIVE: List the infecting pathogens in ventriculitis
OBJECTIVE: Identify risk factors for meningitis due to Listeria monocytogenes
pregnancy
infants less than 1 month
adults over 50
alcoholics with chronic liver disease
immunocompromised
OBJECTIVE: Describe the pathogenesis of community-acquired bacterial meningitis
???
Hematogenous: spread via invasion into bloodstream and evasion of host defenses
Contiguous: infection at a place near CNS (nose or ear) that goes directly to the meninges
OBJECTIVE: Explain the principles of antimicrobial therapy in meningitis
emergent idagnosis
iV admin
adequate CNS penetration
aggressive dosing
bactericidal agents
appropriate spectrum of activity
OBJECTIVE: Design empiric antimicrobial regimens for patients with community- acquired bacterial meningitis based on age, predisposing conditions, and co-morbidities
OBJECTIVE: Define the sub-group of patients who will benefit from adjunctive dexamethasone in the setting of community-acquired bacterial meningitis
all organisms except S. pneumoniae
OBJECTIVE: Modify antimicrobial regimens for patients with community-acquired bacterial meningitis based on infecting pathogen and susceptibilities
OBJECTIVE: Design empiric antimicrobial regimens for patients with healthcare- associated meningitis and ventriculitis based on predisposing factors
OBJECTIVE: List the three most common infectious causes of encephalitis
Herpes Simplex Virus
includes HSV1 (cold sores) > HSV2 (genital warts)
sporadic → any time of the year
treatable
Varicella Zoster Virus
chickenpox/shingles
more in immunocompromised
treatable
West Nile Virus
arbovirus (arthoropod borne - mosquito)
more common in mosquito season (summer into fall)
Enteroviruses
polioviruses, coxsackieviruses, echoviruses, etc
transmitted via respiratory and fecal-oral
summer and fall months
OBJECTIVE: Design empiric antimicrobial regimens for patients with suspected encephalitis
IV acyclovir → diagnostic studies to identify cause → continue for 14-21 days if HSV is confirmed
early treatment is very important
OBJECTIVE: Explain the pathogenesis of brain abscess
infection of brain tissue characterized by a well - vascularized capsule
early infection (1-2 weeks): acute inflammation
late infection (2-3 weeks): formation of necrotic pus → abscess
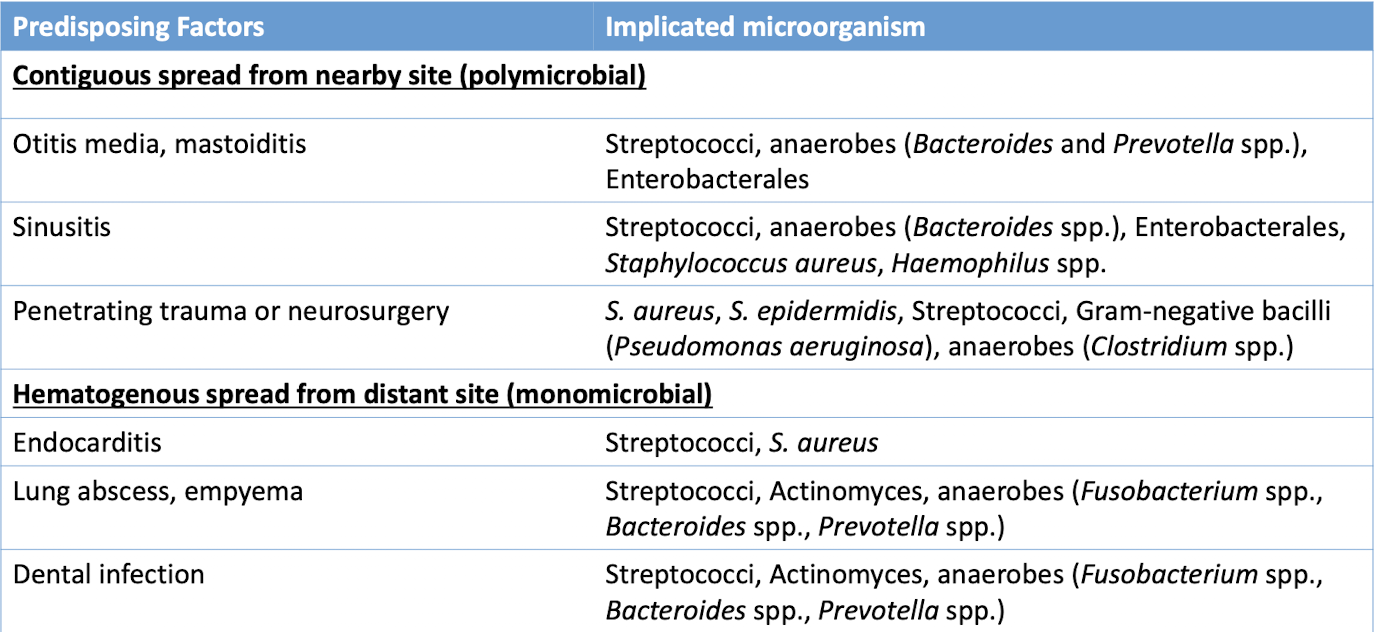
OBJECTIVE: List the infecting pathogens in brain abscesses based on the predisposing factor/source of infection
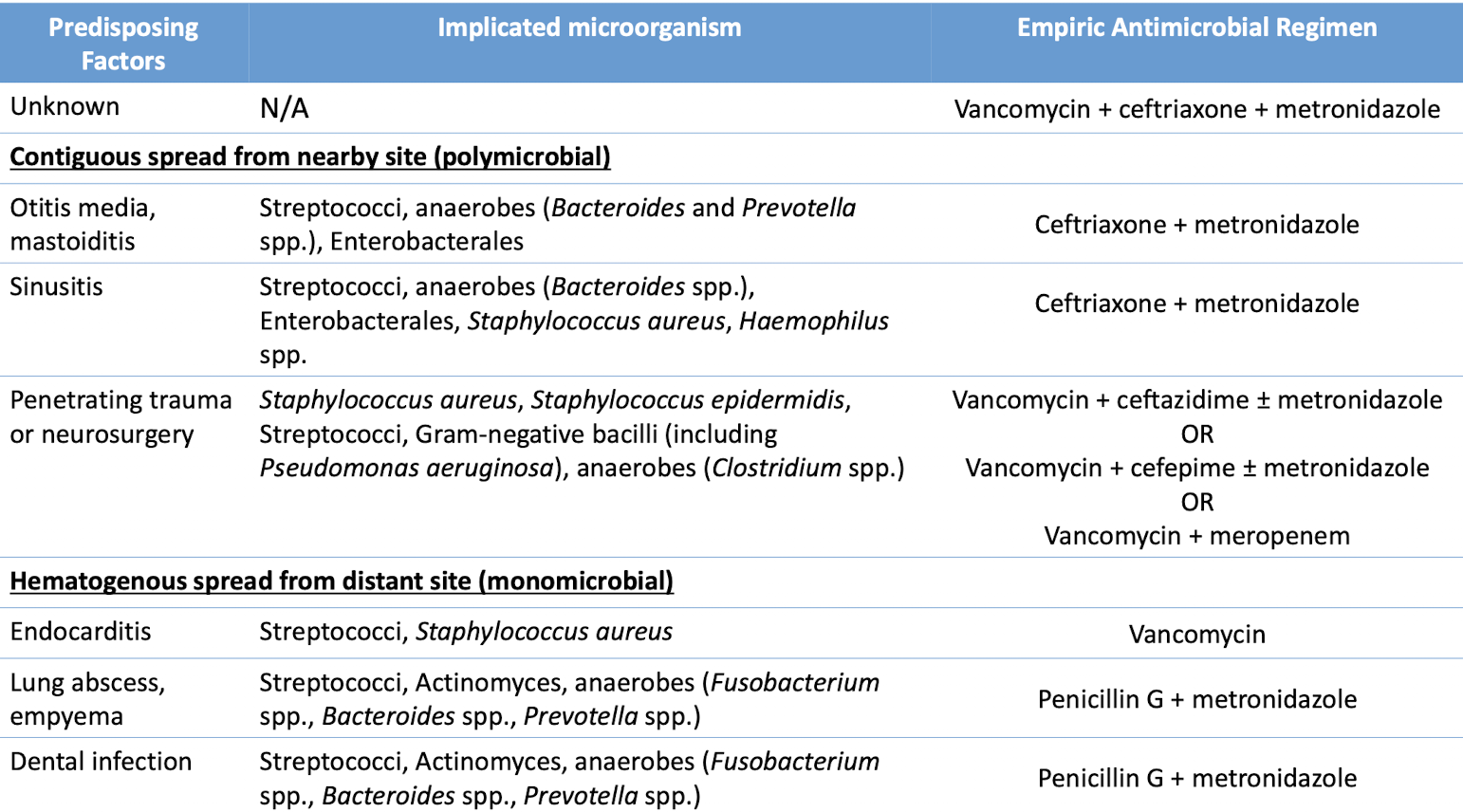
OBJECTIVE: Design empiric antimicrobial regimens for patients with brain abscesses based on the predisposing factor/source of infection
CNS Infections are located
within the cranium or spinal column (meningitis, ventriculitis, encephalitis, brain abscesses) and these are all medical emergencies
Anatomy of the Maters
SKULL
Dura Mater
Arachnoid Mater
under here is the subarachnoid space where csf flows
Pia Mater
BRAIN
Role of brain tissue capillaries
used as a barrier due to its tight junctions and thick glial cells that keeps toxins and byproducts out of the CNS
must be able to overcome these barriers to treat CNS infections
Meningitis Definition
inflammation of the subarachnoid space or CSF
community acquired or healthcare associated
Is there a vaccine for meningitis?
most causative organisms of meningitis are vaccine-preventable
Most common meningitis causative organism
streptococcus pneumoniae
Ventriculitis Definition
inflammation of the ventricles of the brain
Encephalitis Definition
inflammation of the brain tissues
Brain abscess Definition
infection of the brain tissue characterized by well vascularized capsule
Streptococcus pneumoniae
Group B Strep (streptococcus agalactiae)
gram positive
the leading cause of neonatal meningitis → colonizes in GI and genitourinary tract of mothers
Neisseria meningitidis
gram negative
colonizes respiratory tract → very easily transmissible (spread by droplets)
example: Meningitis Belt in Africa
clinical presentation: looks like large bruises
due to leakage of blood outside the blood vessels
Haemophilus influanzea type B
gram neg
respiratory tract
uncommon due to vaccine
Listeria monocytogenes
gram postive
enters via GI - food
Foods assocaited w listeria
unpasteurized milk
soft cheeses
raw produce
deli meat, hot dogs
Risk factors for listeria
(not everyone will get meningitis due to listeria; just ppl w these risk factors)
pregnancy
infants less than 1 month
adults over 50
alcoholics with chronic liver disease
immunocompromise
Meningitis hematogenous vs contiguous spread
Hematogenous: spread via invasion into the bloodstream and evasion of host defenses
Contiguous: infection at a place near CNS (nose or ear) that goes directly to the meninges
Meningitis Clinical Presentation
classic triad
fever
nuchal rigidity (neck)
altered mental status
Meningitis Complications
Systemic (septic shock, disseminated intravascular coagulation, acute respiratory distress syndrome, septic arthritis)
Neurologic (impaired mental status, increased intracranial pressure, seizures, hearing loss)
Initial Meningitis Treatment
(assuming no brain mass)
dexamethasone + empiric antimicrobial therapy
Normal CSF
WBC: <5
Protein: <50
Glucose: 45-80
CSF/blood glucose ratio: 50-60%
Bacterial meningitis CSF
WBC: 1,000-5,000
Type of WBC: neutrophils
Protein: elevated
Glucose: low
CSF/blood glucose ratio: decreased
Multiplex PCR
identifies the causative organisms of meningitis or encephalitis
Meningitis Therapy
adjunctive dexamethasone (decreases inflammation) → empiric antimicrobials (bc its an emergency) → targeted antimicrobials (after receiving susceptibilities)
Limitation of Dexamethasone in Meningitis
decreased inflammation = decreased porousness of BBB = decreased penetration of antimicrobials
When to give dexamethasone
simultaneously with the first dose of antimicrobial OR 20 min before
discontinue if causative organisms are not S. pneumoniae
Agents that will never reach CNS/will not cross BBB
aminoglycosides
1st/2nd gen cephalosporins
doxycycline
pip tazo
Ampicillin dose for CNS Penetrations
2g IV q 4hr
Ceftriaxone Ampicillin dose for CNS Penetrations
2g IV q 12hr
Empiric antimicrobials for 2-50 years old
Ceftriaxone and vanco
Empiric antimicrobials for 50+ years OR any age with risk factors for Listeria
Ceftriaxone, vancomycin, and ampicillin
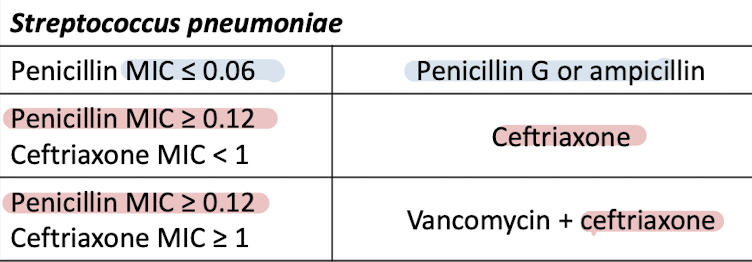
Targeted antimicrobial drug of choice for streptococcus pneumoniae & duration of therapy
duration: 10-14 days
Targeted antimicrobial drug of choice for neisseria meningitdis & duration of therapy
duration: 7 days
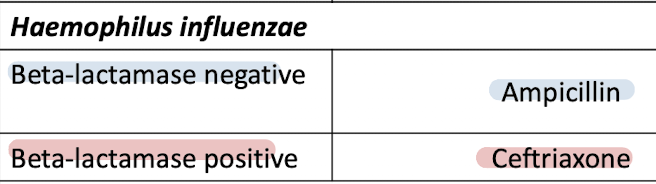
Targeted antimicrobial drug of choice for haemophilus influenzae & duration of therapy
duration: 7 days
Targeted antimicrobial drug of choice for listeria & duration of therapy
duration: 21 days
Targeted antimicrobial drug of choice for group b streptococcus & duration of therapy
duration: 14-21 days
Bacterial pathogen associated with CSF shunts and drains
Coagulase-negative staphylococci (CoNS) Staphylococcus aureus (including MRSA) Gram-negative bacilli (including Pseudomonas aeruginosa) Cutibacterium acnes (formerly Propionibacterium acnes)
Bacterial pathogen associated with neurosurgery and poen/penetrating trauma
Coagulase-negative staphylococci (CoNS) S. aureus (including MRSA) Gram-negative bacilli (including P. aeruginosa)
Bacterial pathogen associated with closed trauma
Streptococcus pneumoniae Haemophilus influenzae Group A streptococcus (S. pyogenes)
Clinical Presentation of Hospital acquired meningitis and vasculitis
Fever, Headache, Nausea, Lethargy, Change in mental status, Seizures
Diagnosis of of Hospital acquired meningitis and vasculitis
Approach to Treatment of Hospital acquired meningitis and vasculitis
Empiric antimicrobials → targeted antimicrobials → intraventricular/intrathecal antimicrobials (only used when pt fails to respond to IV)
Treatment for CSF shunts and drains
Vancomycin + cefepime
Vancomycin + ceftazidime
Vancomycin + meropenem
Treatment for neurosurgery
Vancomycin + cefepime
Vancomycin + ceftazidime
Vancomycin + meropenem
Treatment for open/pentraring trauma
Vancomycin + cefepime
Vancomycin + ceftazidime
Vancomycin + meropenem
Treatment for closed trauma
Vancomycin + ceftriaxone
make flascards for slide 55
Intraventricular/intrathecal antimicrobials
direct instillation of antimicrobials into the CNS
Encephalitis Clinical Presentation
fever, headache, brain dysfunction → altered levels of consciousness, seizures, altered behavior, speech or movement disorders, etc
Encephalitis diagnosis
PCR, viral cultures, antibodies
Brain abscess clinical presentation
Brain abscess diagonsis
Brain CT
Brain abscess treatment
antimicrobial + neurosurgery to drain it
Brain abscess approach to therapy
imaging of brain abscess → empiric antimicrobial therapy → CT guided neurosurgery → targeted antimicrobial