

cardiology
Heart failure
It is a clinical syndrome that can result from any structural or functional cardiac disorders that impairs the ability of the ventricles to fill with or eject blood. There are 2 arteries: pulmonary artery and aorta and 2 veins: vena cava and pulmonary vein. The pulmonary artery divides into two transports deoxygenated blood into the heart.
If the load on the heart becomes too much, or if the organ is getting old, when the heart does not cope with the load this results in heart failure. The heart is not pumping as well as it should. Usually the heart has been weakened by an underlying condition such as; blocked arteries, high blood pressure or heart valve abnormalities. Heart failure can be presented in two forms, anabolic- the heart no longer has the ability to eject blood effectively or diastolic in which the ventricles are unable to be filled properly. Narrow arteries result in lack of circulation, this results in elevated blood pressure. Each valve has a different mechanism in the way they work. If the valve regulating inlet leaks or is very narrow, the heart needs to work harder to pump blood.
When this happens there is not enough perfusion of oxygenated blood into the organs and blood will accumulate in the venous system. This results in very high pressure exerted in the veins. There is also an increased pressure on the alveoli and this results in shortness of breath. It is important to identify what is causing this failure as the treatment will be different.
Left ventricular failure occurs when there is dysfunction of the left ventricle causing insufficient delivery of blood to vital body organs. In systolic failure, the heart loses its ability to contract or pump blood into the circulation while in diastolic failure the heart loses its ability to relax because it becomes stiff. The heart cannot fill properly between each beat. In both types, blood may back up in the lungs causing fluid to leak into the lungs (pulmonary edema). Systemic pressure is transmitted to the right side organs (liver, lower limbs) which will become congested. Fluid may also build up in tissues throughout the body (edema). The main giveaways that a person is suffering from heart failure are symptoms such as shortness of breath and swelling of the ankles. Shortness of breath can occur during any time of the day, however it is more acute at night. This phenomenon is known as orthopnea. Here shortness of breath is experienced when lying down. During the day, the fluid is situated at the base of the lungs, however when a person is lying down, fluid distributes all over the surfaces of the alveoli and drowns them. This phenomenon is known as paroxysmal nocturnal dyspnoea. This is a sensation that wakes the patient up after 1-2 hours and is usually relieved in the upright position.
Right ventricular failure usually occurs as a result of left heart failure. This can also occur due to lung disease or blood clots to the lung (pulmonary embolism). Patients that suffer from this condition usually have massive veins and an enlarged liver. Cor pulmunare is a condition that causes the right side of the heart to fail. Heart failure is a chronic condition. Initially the heart tries to compensate for the loss in pumping function by developing more muscle mass, enlarging and pumping faster. Initially, the disease is stablised however, if there is an infection or stressor, it will lead the patient into heart failure. Any heart disease can cause heart failure, even systemic diseases which are not directly affecting the heat such as lung diseases or if the thyroid gland is working too fast. Diseases of the heart that eventually lead to heart failure include: high blood pressure, abnormal heart valves, atrial fibrillation, cardiomyopathies, congenital heart defects. Non cardiac diseases that induce heart failure include:
severe lung disease,
Anaemia- not enough RBC to carry oxygen, heart beats faster and can become overtaxed with the effort
diabetes and
Hyperthyroidism- body metabolism is increased and overworks the heart
Abnormal heart rhythm- if the heart beats too fast, too slow or irregular it may not be able to pump enough blood to the body
Another reason for oedema is because kidneys respond to low perfusion. They regulate the Na and water levels of the body. The body will retain water and sodium. The kidney cannot distinguish profusion from heart failure or dehydration and the RAAS system starts to retain Na and water. This increases the workload on the heart and causes major oedema. Physical signs of heart failure include- increased heart rate, raised JVP, crackles in the lung bases, enlarged liver, ankle oedema.
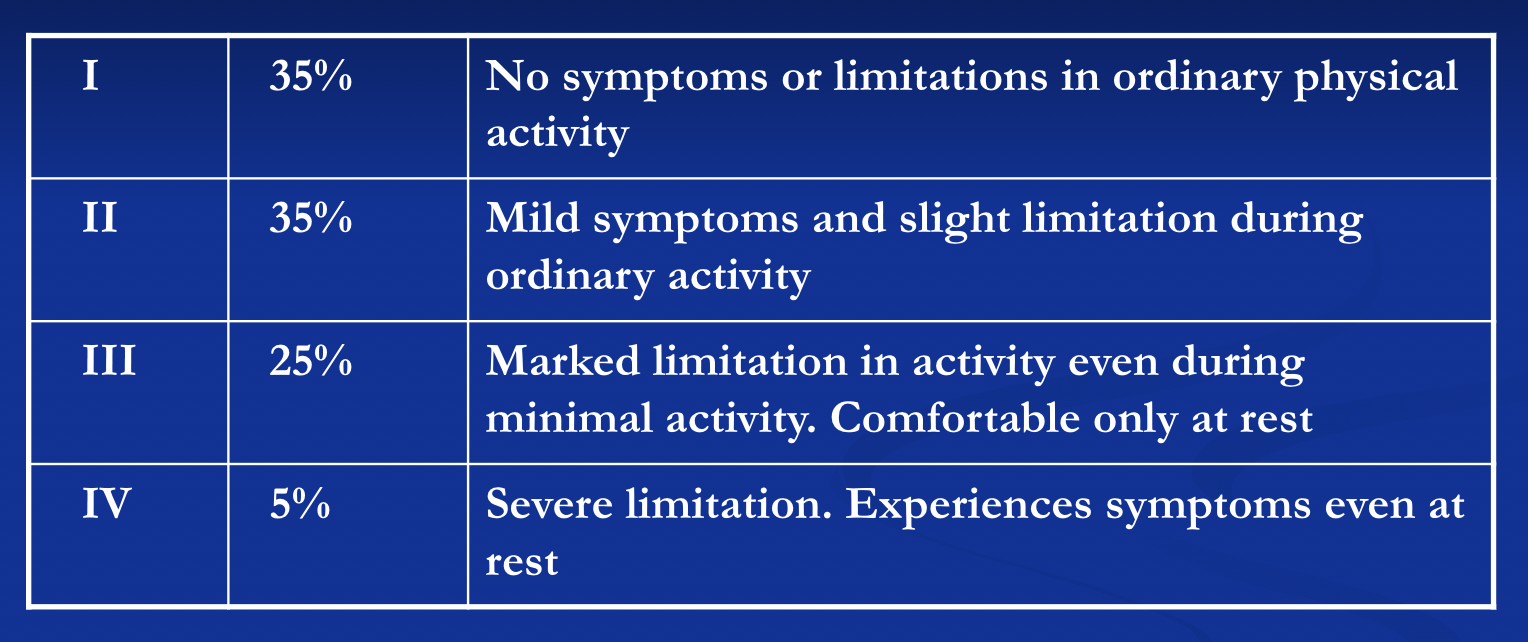
If the heart rate is increased, profusion will also increase raising the heart rate however, oxygen consumption will be decreased. Patient eventually dies from pulmonary oedema which results in hypoxia which is the number 1 killer of all diseases. Hypoxia makes the person feel anxious, distressed and sweaty. The new York Heart association created a criteria to classify heart diseases.
The main 4 investigations used to assess heart failure are: ECG, chest X ray, echocardiogram and an angiogram. An echocardiogram is the best method for diagnosis. With an ECG, you are not able to diagnose heart failure but it will indicate what leads to heart failure. The way this works is by measuring the walls of the muscles during diastole and systole. With a chest X ray, one can determine if the size of the heart is enlarged (cardiomegaly), pulmonary congestion, alveolar oedema and pleural effusion. With an echocardiogram, congenital defects can be observed, determine if the heart is affected by endocarditis and make sure that the dimensions are correct. In infective endocarditis, the heart valves are infected.
Drugs used for treatment work mainly by 3 mechanisms: excreting urine hence reducing the blood volume, target the renin angiotensin by using a renin angiotensin inhibitor and by reducing the heart rate via beta blockers. The three main classes of drugs used to treat heart failure are: diuretics, ACE inhibitors, and beta blockers. Diuretics are further divided into 3 divisions: thiazides, K- sparing, loop diuretics. In the medical industry, loop diuretics are over used and these often lead to kidney failure. Thiazides on the other hand are less powerful, in diabetic patients this drug can worsen diabetes. Both loop and thiazides excrete too much K and Mg. This can lead to hyperuricemia, hypotension and ototoxicity. Diuretics that retain K are also called anti aldosterone drugs that target the aldosterone production. Aldosterone inhibitors such as spironolactone are competitive antagonists of the aldosterone receptor. With a reduction in aldosterone, Na and water are retained while magnesium and K are excreted. Spironolactone are not used in hyperkalemia or in renal insufficiency. It is also important to continuously monitor serum potassium.
Ace inhibitors are medications that help to relax veins and arteries to lower blood pressure (end in -pril). These work by blocking the enzyme that converts angiotensin 1 to angiotensin 2. ACE-1 can cause hypotension (1st dose effect), worsening of renal function, hyperkalaemia, cough, and angioedema. These are contraindicated when there is narrowing of the renal arteries (stenosis), hyperkalaemia, severe hypotension, and pregnancy. Angiotensin- 2 receptor blockers are indicated in patients who are intolerant to ACE- 1.
Beta blockers are commonly thought of as contraindications of heart failure. It works mainly by reducing the heart rate and therefore reducing the energy expenditure. Some adverse effects of beta blockers include: hypotension, worsening of heart failure, bradycardia, and asthma. These are contraindicated in asthma, AV block (unless pacemaker), symptomatic hypotension. These are suitable for patients with diabetes
Digitalis are types of medications used to treat several heart conditions. Their mode of action to on the sodium- potassium ATP-ase of the myocyte. It reversibly inhibits the ATPase resulting in increased intracellular sodium levels. The build up of intracellular sodium levels leads to a shift of sodium extracellularly though another channel in exchange for calcium ions. These help to improve symptoms, modest reduction in hospitalisation however it does not improve the survival rate. These are indicated in atrial fibrillation to slow down the AV conduction. These are used when there is no adequate response to ACE-1, diuretics and beta blockers. Can also be used in combination with ACE-1 and diuretics if symptoms persist. These are contraindicated during digoxin toxicity, AV block, and arrhythmias.
Vasodilators can either work on veins (nitrates) or arteries (hydralazine). If you dilate arteries, there is less blood pressure and the heart will pump less. If the veins are dilated, there is less blood therefore less pressure is going to the heart and the workload is overall reduced. Nitrates are good in acute heart failure, CHF with myocardial ischaemia, orthopnea and paroxysmal nocturnal dyspnea
Ischaemic heart disease
Most of the blood supply is going into the left coronary artery. This is further divided into two. If the right coronary artery is blocked the person will live, however if the left side is blocked, this is fatal. The LAD is the most important artery and if blocked, it is important to try to open any blockages. The heart is a muscle which needs oxygen. If the supply is less than the demand chest pain is experienced which is known as angina. Anoxia is when no oxygen reaches the tissues. This causes ischaemia of tissues. Supply is mainly affected by the diameter of the coronary arteries. Blood loss could also precipitate angina.
The person’s diet has a direct effect on the formation of an atheroma. Heart vessels can also be narrowed when the diet consists mainly of junk food. Lipid deposition causes an inflammatory response. The endothelial lining might rupture which will lead to a heart attack. Narrowing of the lumen can be caused either by longitudinal plaque formation or formation of a lump. Symptoms start to emerge only when the demand of oxygen exceeds the supply or when the plaque ruptures and the endothelium recognises it as a foreign body. This will attract platelets to the site which will form a blood clot. This clot will obliterate the lumen and will cause a heart attack. An angioplasty (molla) is a stand which is placed into the blocked vessel and this will squash the plaque out.
Angina occurs when there is narrowing of the artery but no plaque is forms. It is the stable form when it is provoked by exercise and relieved by rest.Patients suffering from heart failure feel sharp pain in their chest which is compressive and often radiates to the arms and jaw. Stable angina is short lived and is relieved by rest while unstable angina is prolonged, is not relieved by resting, and does not respond to glyceryl trinitrate (GTN). In acute coronary syndrome, there is rupture of the plaque and it is not relieved by rest. This is further divided into two forms: complete occlusion STEMI and NSTEMI. In the STEMI situation, they do an angioplasty immediately this is a very urgent matter while in NSTEMI they do it they following day. Heart vessels need to be opened up urgently as they do not have the ability to regenerate and will cause death of muscle. Some of the plaques formed are more vulnerable than others. This all depends on how thick the endothelial lining is.
The most important thing when viewing a patient is a thorough history. Take their medical and social history to look for further risk factors. Such risk factors include: diabetes, hypertension, hyperlipidaemia, and smoking.
Various methods can be implied to diagnose heart failure and angina. Patients presenting to hospital are usually acute. An ECG is usually conducted to diagnose a myocardial infarction. Blood test can also be taken and the values of CK and troponin are checked. To diagnose ischaemic heart disease, a stress test is conducted. If you are sure that there is narrowing of an artery, an angiogram is carried out. An ST elevation on an ECG indicates MI and an ST depression indicates acute ischaemia. Troponin is a very sensitive enzyme and thus it causes a lot of false positives. CK is an early marker. It is released during muscle damage specifically cardiac muscles. Stress ECG is a screening tool which is used to identify patients requiring an angiogram. This test is used in stable patients. As the heart rate increases, so does the oxygen demand and the ST part is checked. If ST depression is positive, take an angiogram. Having said so, the specificity and sensitivity of this method is not very good. An MIBI scan is better than the treadmill test. In this test, an isotope is injected and the different colour changes will show different areas of ischaemia. This will help clinicians to determine if there is healthy muscle of ischaemia. Angiogram is the best test to identify the anatomical location of plaque, how severe the situation is and the plan management.
There are different types of drugs which target different parts of the pathological process. Asprin is used in stable diseases while clopidogrel is used in unstable. Nitrates, beta blockers, ACE inhibitors, calcium antagonists and statins are among the drugs prescribed for heart failure. Nitrates work by reducing the oxygen consumption, these are often prescribed for acute chest pain and patient with liver diseases as it bypasses the liver. This category is further subdivided into: oral nitrates, transdermal nitrates and intravenous nitrates.
A PCI and a CABG are indicated in severe coronary artery stenosis. A PCI is done for single lesions while a CABG is done when there are multiple severe lesions. When a patient undergoes these treatments, a lot of antiplatelet drugs are prescribed. CABG is the best out of the two methods. Acute coronary syndrome is a term used to describe a range of conditions with rudden, reduced blood flow to the heart. This includes all cases of prolonged, resting chest pain. The main treatment is to provide oxygen, IV nitrates, heparin and maximised oral treatment. If an angioplasty cannot be performed, opt for thrombolytic therapy.
Hypertension
Hypertension is a silent killer which often represents itself as a headache. Most primary hypertension is essentially hereditary and around 4-5% of the secondary HT have kidney problems. There are several risk factors that predispose a patient to this disease such as: gender, genetics, certain ethnic groups, and environmental factors such as a sedentary lifestyle. The two main components that are affected are mainly the peripheral resistance and the cardiac output.
Secondary high blood pressure is high pressure that is caused by another medical condition. It can be caused by conditions that affect the kidneys, arteries, heart or endocrine system. Any kidney disease will elevate the heart pressure and sometimes kidney diseases are caused due to hypertension. This makes it difficult to determine the primary and the secondary problem. Other factors that cause an elevated blood pressure are endothelial dysfunctions. Renin is secreted when blood pressure is too low thus activating angiotensin II to increase blood pressure and vascular resistance. Abnormal activation of RAAS leads to chronic hypertension, cardiac failure and kidney conditions. Glands produce hormones and excess hormones lead to the development of tumours. Atherosclerosis is the main reason for heart pressure. Every artery of the body will narrow and this causes damage to all the arteries of the system. Hypertension causes different complications in different organs such as: hemorrhage and stroke in the brain, retinopathy in the eyes, peripheral vascular disease in the arteries, renal failure and proteinuria in the kidneys, LVH, CHD, and CHF in the heart.
There are no symptoms which are directly associated with hypertension; this is what makes it a silent killer.
When taking the medical history, it is important to look for symptoms that might be caused due to hypertension such as: headache, dizziness, pressure on the chest. The usual risk factors that predisposes a patient for an elevated blood pressure include: diabetes, lipids, smoking and obesity. Clinical signs of uncontrolled hypertension include headaches, blurred vision (papilloedema), shortness of breath (pulmonary oedema) and chest pain (aortic dissection). When managing hypertension it is important to diagnose secondary hypertension, assess end organ disease and look at risk factor modification. Firstly it is important to opt for non pharmacological management such as exercising, controlling diabetes, treating any underlying disease, improving the diet and reducing smoking. However drugs can also be prescribed. To test how bad things are, the urine is checked for proteins and an ultrasound is carried out to check for creatinine as these levels tend to go up at an advanced stage. It is also important to check the cortisol levels and catecholamines.
ABCD are the drugs which are used in hypertension. These include: ACE inhibitors, Beta blockers these target the sympathetic chain, Calcium channel blockers these relax the muscle layer of the artery and cause ankle oedema and Diuretics which work by reducing the blood volume.
ACE inhibitors work by blocking the metabolism of bradykinin. Angiotensin II which comes from the kidney, retain sodium and water for dehydration, this is blocked to reduce the blood pressure. However, if ACE inhibitors accumulate these cause inflammation in the lungs which result in a dry cough. A2 receptor blockers are used after the dry cough is formed.
Beta blockers block the heart rate. These decrease the heart rate and the force of contraction which eventually results in a decreased cardiac output. One main disadvantage of beta blockers is that they cause bronchoconstriction which may be fatal in people who suffer from asthma and can also induce pain in the legs and cause oedema. They can lead to further heart failure and bradycardia (slow heart rate).
Calcium channel blockers block the calcium channel which result in vasodilation hence decreasing the blood pressure. The most common Calcium channel blocker is amlodipine. There are other Ca channel blockers such as verapamil and diltiazem which also reduce the contractility. The adverse effects of this class is that they can cause oedema, constipation, bradycardia and heart failure.
The primary site of action for diuretics is in the nephron. There are 3 types of diuretics: thiazides, K- sparing and loop diuretics. Thiazides are used as a first option. The thiazides inhibit the active exchange of Cl-Na in the cortical segment of the ascending look of Henle. The K- sparing inhibit the reabsorption of Na in the distal convoluted tubule and collecting duct. Loop diuretics inhibit the exchange of Cl-Na-K in the thick segment of the ascending loop of Henle. Thiazides need to be used with caution as they have a tendency to: worsen diabetes, cause hyponatraemia and hypokalaemia. With K sparing these can cause hyperkalaemia and C/i renal failure while look diuretics may worsen renal function.
Atrial fibrillation and diseases of heart valves
In total there are 4 valves in the heart. The annulus is the part which keeps the valves in place as the rest of the heart is built around the valves. The sinus node sens impulses (P wave) to the left atrium, right atrium and the AV node. The AV node transmits impulse to both ventricles. Atrial fibrillation occurs when electrical foci in the atria produce fast irregular impulses overriding the sinus node. These fast atrial impulses are transmitted by the AV node to ventricles which will produce a fast and irregular heart beat. The AV node determines how many of the atrial impulses are transmitted therefore determining the ventricular heart rate.
Atrial fibrillation is the most common arrhythmia as it is a disturbance of the electrical impulses going to the atria. In fibrillation, the heart is contracting but no blood is flowing. This causes blood to stagnate in the appendage of the atria. This results in the formation of a cloth which fill cause a stroke. When looking at an ECG there is no P wave.
Some of the causes of atrial fibrillation include: structural heart disease such as HT, IHD, VHD, and CHD or even non cardiac diseases such as hyperthyroidism, pneumonia, COPD and hypoxia. Elevated blood pressure is the most common reason for atrial fibrillation. Stasis in the left atrium can cause a cloth that embolises and cause a stroke or can form in other areas such as the GIT or limbs. Another compilation is heart failure as a fast heart beat reduces ventricular filling which leads to cardiac failure.
High flow valves are the mitral and the aortic valve. These result in left ventricular failure. These all result in either: degenerative calcification, post rheumatic fever, endocarditis or valve defects which may be congenital. Rheumatic fever directly affects the valve, this infection of the valves leads to endocarditis. Diseases of the aortic valve leads to aortic stenosis. The valve opening is small due to stiff or fused leaflets. The valve can also be narrowed due to heart failure or left ventricular hypertrophy. Another diseases is aortic regurgitation. In this disease the valve does not close tightly and the valves start to leak.
Mitral valve disease include: mitral stenosis and mitral regurgitation. In mitral stenosis, the LV is not filled completely which results in heart failure. In mitral regurgitation, the valve leaks blood into the LA which also leads to heart failure. For these diseases, the thyroid function is checked and 2 types of drugs are prescribed these include anticoagulants, rivaroxaban but the best drug to prescribe is beta blocker.
Endocarditis is inflammation of the endocardium, this includes the heart valves. This is caused by platelets as they start ticking to the valves. They stick due to abnormalities of the valve. These abnormalities are either congenital, caused by calcification or because the patient has a prosthetic valve. As the platelets start sticking together which results in an abnormal flow. The combination of bacteria, platelets, fibrin and inflammatory cells form a vegetation. This prevents the opening and closing of the valves. Endocarditis can occur after an extraction. The patient gets a bacteremia which causes endocarditis hence why antibiotics are given. Nowadays it is not as common to get an endocarditis from an extraction, but are coming from the gut, drug addicts or an infected prosthetic heart valve. Vegetations can embolise and form an abscess. Staph aureus cases acute endocarditis and abscess while step viridancs causes subacute endocarditis. Murmurs can be a sign of endocarditis. Other signs of AF include palpitations, dizziness, shortness of breath. It is important to look for irregular pulse, hemiplegia (embolic stroke) and thyroid goitre. Symptoms of endocarditis include: fever, chills or night sweats, weight loss, fatigue, shortness of breath, anaemia, heart murmur. Endocarditis can cause Osler;s nodes, splinter haemorrhages and janeway lesions. Endocarditis is diagnosed with an echocardiogram and the same drugs used for atrial fibrillation are used for endocarditis. Diagnosis is further confirmed by a positive blood culture and viewing vegetations on Echo.
AF is treated by drugs which slow down HR- beta blockers, digoxin, verapamil. Endocarditis is managed by antibiotics or surgery.