Tags & Description
Outline 4 types of angina
1. Decubitus angina: pain worse when lying down, stable, atherosclerotic
2. Prinzmetal's or variant angina: ST elevation due to coronary vasospasm
3. Syndrome X: ST depression on exercise ECG but normal angiogram, sign of microvascular disease
4. St. Vincent's angina: pharyngitis caused by ulcerative gingivitis
Other than atherosclerosis, what are 2 causes of angina?
Aortic valve disease
Cardiomyopathy
List the risk factors for coronary disease
Hyperlipidaemia
Diabetes
Smoking
Hypertension
Obesity
CKD
Outline the investigations for coronary artery disease
Anatomical: CTCA (+ calcium score), invasive coronary angiography
Functional:
exercise stress test/ echo
myocardial perfusion scan
cardiac MRI with stress perfusion
exercise ECG
Outline the treatment of angina
Treat risk factors
GTN spray for acute relief
1st line BB's or CCB
2nd line long acting nitrates (if GTN responsive) or nicorandil, ivabradine or ranolizine
75 mg aspirin + statin
Consider CABG and PCI
Outline the A-E steps of assessment
Airway- own, patent
Breathing- RR, saturation (pulmonary oedema due to LVF? hypoxia)
Circulation- HR/BP (bradycardia= inferior MI, hypotension= cardiogenic shock/RV infarction, murmur)
Disability- GCS, glucose
Exposure- pain, inspection, bleeding, temp
List the causes of high serum troponin
Myo/pericarditis
CKD
PE
Cardiomyopathy
Atrial fibrillation/tachyarrhythmia
List the ECG changes in acute coronary syndrome
ST segment deviation (elevation or depression)
T wave inversion
Bundle branch block (delayed QRS)
Localisation
How do you look for ST segment deviation on an ECG?
Locate J point- inflection point between QRS and following segment
ST segment can be above or below point
Outline the immediate symptomatic management of ACS
Pain- morphine + nitrates
O2 if hypoxic
Outline the prognostic treatment for ACS
Dual antiplatelet therapy: aspirin (lifelong) + P2Y12 inhibitors
Atorvastatin 80mg
Cardio-selective BB (bisoprolol)
ACE inhibitor (ramipril) or ARB
PPI (if above 65yrs and/or history of GORD/ peptic ulcer disease/ dyspepsia etc)- aspirin can cause stomach bleeds
Describe the definitive management of ACS
Coronary angiography
if STEMI, do immediately
if NSTEMI, do within 72 hrs
PCI
Emergency CABG
Define ACS
Encompasses range of conditions including STEMI, NSTEMI and stable angina that are all due to sudden myocardial ischaemia
Outline the complications of ACS
DARTH VADER
Death
Arrhythmia- sinus brady, SVT, heart block, V fib
Rupture (free ventricular wall, ventricular septum + papillary muscles)
Tamponade
Heart failure
VSD
Aneurysm of ventricles- seen as persistent ST elevation without chest pain
Dressler’s syndrome- pleuritic pain, pericarditis, fever, pericardial effusion; 10-14 days after MI
thromboEmbolism (mural thrombus= attached to endocardium)
Recurrence/ mitral Regurgitation
Compare infarction vs injury
Myocardial injury= trop > 99th percentile e.g. myocarditis
Infarction= injury due to myocardial damage from ischaemia e.g. MI
Describe Takotsubo's cardiomyopathy
Presents as STEMI with heart failure symptoms + chest pain
Catecholamine mediated stress CM in post-menopausal women
Myocardial stunning
Findings: unobstructed coronaries + transient LV impairment with sparing of top of ventricle
AKA broken heart syndrome
Myocardial INJURY
Distinguish between type 1 and 2 MI vs myocardial injury
Type 1: acute ischaemia, atherosclerosis + thrombosis
triggered by plaque rupture/erosion :. requires PCI, CTCA
Type 2: acute ischaemia, O2 supply + demand imbalance e.g. severe hypertension, sustained tachyarrhythmia
Myocardial injury: without acute ischaemia e.g. acute heart failure, myocarditis
:. treat underlying causes
Outline the signs and symptoms of mitral regurgitation
Symptoms:
dyspnoea
fatigue
RHF (ankle oedema, abdomen distension)
Signs:
full volume pulse
AF
pansystolic murmur
tachycardia
ST depression
bilateral crackles on auscultation (pulmonary oedema)
Outline the management of severe mitral regurgitation as a result of flail posterior mitral valve leaflet
Furosemide- for pulmonary oedema
LMWH + IV amiodarone- for AF
Referred for urgent surgery
Outline the causes of mitral regurgitation
Congenital
Rheumatic
Myxomatous degeneration
Endocarditis
CAD
CM (dilated LV)
AF (dilated LA)
CREAM CupCake
Describe the pathophysiology of mitral regurgitation
LV volume overload-> increased LV emptying
Increased LA pressure
Increased LV filling pressure
Increased LV end diastolic damage
LV stretches-> failure
Outline the causes of mitral stenosis
Rheumatic fever
Severe annulus calcification
LA myxoma (benign tumour)/thrombus
Congenital
Outline the signs and symptoms of mitral stenosis
Dyspnoea
Palpitations
AF
Mitral facies (flushed cheeks, cyanotic lips)
Opening snap (mitral valves tensing + go into LV due to high pressure
Mid-diastolic rumbling murmur when lying on left
Presystolic murmur
Describe the pathophysiology of mitral stenosis
Blood unable to flow to LV due to leaflet rigidity
Increased LA pressure to maintain CO
LA dilation-> AF
Increased pulmonary pressure-> Outline the causes of mitral regurgitationpulmonary congestion
R + LHF
Describe the pathophysiology of aortic stenosis
Progressive narrowing of valve due to calcific degeneration
Compensatory LVH to maintain SV
Pressure overload -> LVF (SOB, angina, syncope)
Outline the management of aortic stenosis
Surgical or percutaneous valve replacement
Poor prognosis if symptomatic
Describe the pathophysiology of aortic regurgitation
AR leads to compensatory LV dilation + hypertrophy to maintain SV
LV dilation -> LVF (no LV dilation in acute AR)
List the causes of aortic regurgitation
Valvular:
infective endocarditis
rheumatic
degenerative
bicuspid AV
trauma
Aortic root:
hypertension
dissection
aortopathy e.g. in Marfan's
Outline the signs and symptoms of aortic regurgitation
Early diastolic murmur
left sternal edge
leaning forward
end expiration
Wide pulse pressure (collapsing due to increased SV)
Outline the signs and symptoms of tricuspid regurgitation
Ascites
Raised JVP
Peripheral oedema
Abdo pains
Hepatomegaly (liver congestion)
Define heart failure
The inability of the heart to generate a sufficient CO to meet metabolic demands
WITHOUT an increased filling pressure
This is secondary to an underlying cause e.g. CAD and hypertension
Describe chronic HF
Breathlessness with impaired exercise tolerance
Slowly progressive + had periods of acute decompensation (suddenly worse)
State of fluid retention and overload
Describe acute HF
Can be dramatic with flash pulmonary oedema
Or gradual deterioration of chronic HF due to
fluid accumulation
low exercise tolerance + fatigue
orthopnoea + nocturnal dyspnoea
Compare systolic and diastolic HF
Systolic: HR with reduced ejection fraction (HFrEF) or mildly reduced (HFmrEF)
Normal EF= ABOVE 55%
Diastolic: HF with preserved EF (HFpEF)
stiffness of ventricular wall
impaired filling
reduced CO
echo shows LVH, LA dilation + abnormal relaxation
Compare high output HF and low output HF
High output:
heart overworked
can be physiological (athletes, pregnant) or pathological (sickle cell, thyrotoxicosis)
Low output:
capillary refill slow
increasing breathlessness
List the top 3 causes of heart failure
Ischaemic heart disease (35-40%)
Dilated CM (30-35%)
Hypertensive heart disease (15-20%)
Other- valvular disease, HCM, uncontrolled tachyarrhythmias, viral myocarditis, COPD
Outline the signs and symptoms of heart failure
Symptoms:
breathlessness (on exertion or at rest, orthopnoea, paroxysmal nocturnal dyspnoea)
fatigue
reduced exercise tolerance
palpitations
angina
Signs:
raised JVP
3rd heart sound
pulmonary crepitations
hepatomegaly
peripheral/sacral oedema
cachexia (weight loss/wasting, loss of appetite)
Describe the 4 classes of heart failure (NYHA)
1= no symptoms
2= symptoms on exertion
3= symptoms on minimal exertion
4= symptoms at rest
Outline the possible investigations for heart failure
Routine bloods- FBC, iron, glucose, cholesterol, Ig's, BNP, uric acid
ECG- BBB, STEMI
CXR- pulmonary oedema
Transthoracic echo
Cardiac MRI
Outline the management of heart failure
ACUTE
-high flow oxygen (MONA- morphine, oxygen, nitrate/GTN, aspirin)
furosemide if fluid overload
ECG monitoring
ventilatory support if needed
find cause
CHRONIC
prevent decompensation
maintain or improve symptoms
increase longevity
device (pacemaker, implantable cardiac defibrillators) or surgical therapy
drug therapy- BBs, ARB, ACEi
LVAD (left ventricular assist device) carried in backpack
List the most common causes of secondary hypertension
Primary kidney disease
Primary aldosteronism
Renal artery stenosis
Pheochromocytoma (vascular tumour of adrenal medulla)
Cushing's
Obstructive sleep apnea
Coarctation of aorta
Drugs- NSAIDs, contraceptives, antidepressants
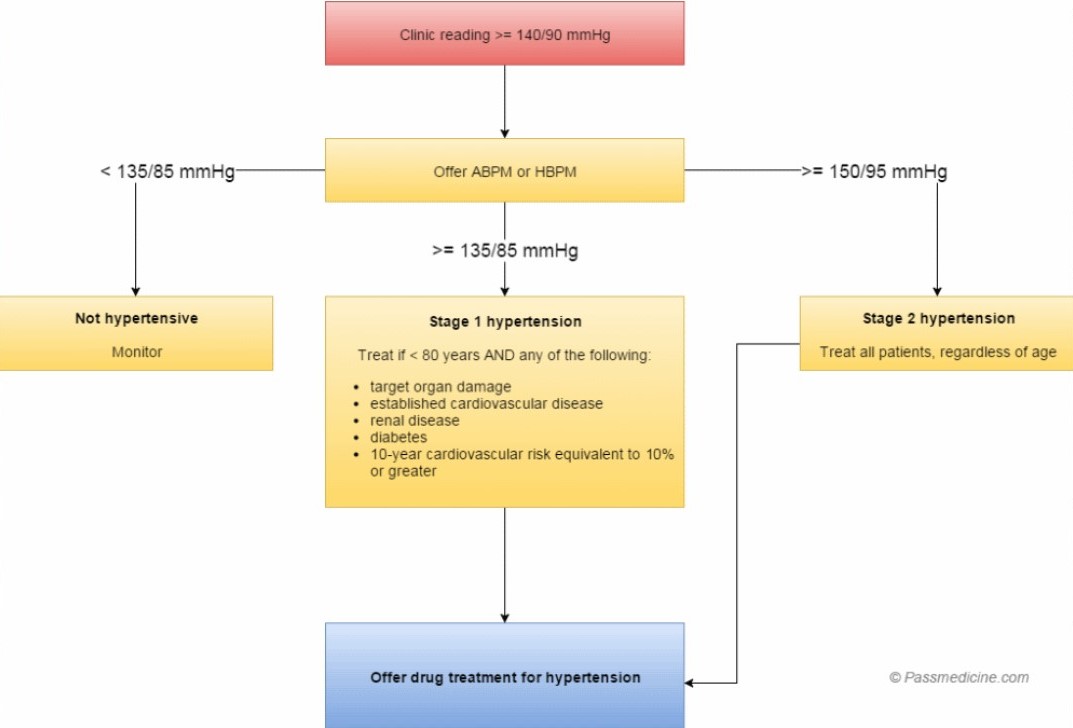
What are the diagnostic values for hypertension?
Clinic BP 140/90
ABPM/home monitoring (day time) 135/85
Outline the management of hypertension
ACD D(squared)
A= ACEi (dry cough) or ARB
C= CCBs e.g. verapamil
D= thiazide diuretics
D^2= loop diuretics e.g. spironolactone (oestrogen side effects e.g. gynaecomastia)
Which antihypertensives are specific to pregnancy?
Labetolol
Methyl dopa
Nifedepine
Outline the assessment of primary tachycardia
Assess using A-E approach
Monitor O2 saturation + give O2 if needed
Adverse features?
e.g. shock, syncope, myocardial ischaemia, HF
If unstable-> synchronised cardioversion shock then specialist + amiodarone
If stable- is QRS narrow (<0.12ms)?
Is rhythm regular?
Describe supraventricular tachycardia and list the 3 types
Tachycardia that originates above the ventricles e.g. atria
Atrial fibrillation/flutter/tachycardia
Atrio-ventricular nodal reentrant tachycardia (AVNRT)
Atrio-ventricular reentrant tachycardia
Which drug can be used to treat AVNRT and AVRT?
Adenosine 6mg
Both conditions affect nodes, interrupted with drug
Describe broad complex tachycardia and give an example
Occurs when ventricular activation is not via normal specialised conduction system e.g. SAN
E.g. ventricular tachycardia where the activation comes from within ventricles + distribution is not even
Compare acute pericarditis and STEMI ECGs
Pericarditis- saddle shaped T wave inversion (smiley face)
STEMI- ST depression (sad face)
List the 4 Plasmodium agents that cause malaria
Most common:
Plasmodium Vivax
Plasmodium Falciparum (most lethal, drug resistant)
Less common:
Plasmodium Malariae (mildest)
Plasmodium Ovale
Outline the clinical features of malaria and its major risk factors
Clinical features:
fever
headaches, muscle aches, diarrhoea or vomiting
Risk Factors:
foreign travel within last 12 months
pregnancy status
immunocompetence status (HIV, cancer, transplant recipients)
drug history (previous prophylaxis, allergies, potential drug interactions)
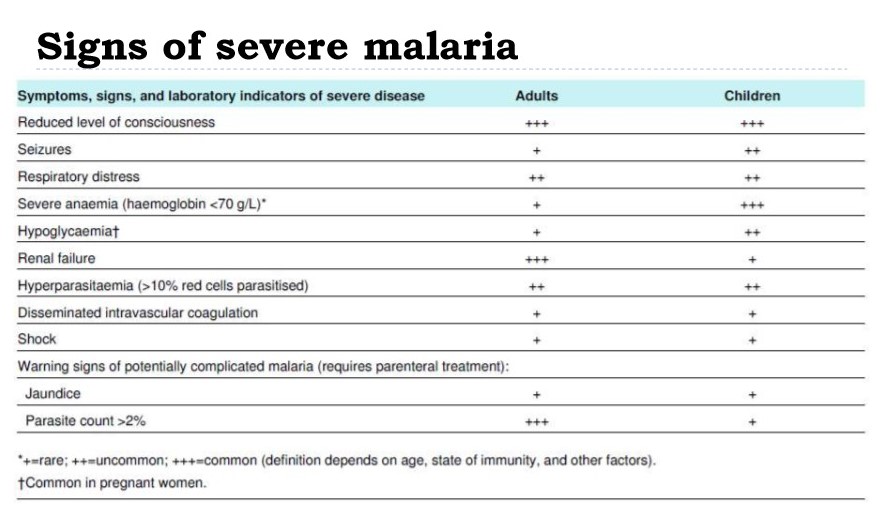
List the signs of severe malaria
List 4 antimalarials and their mechanism of action
Quinoline derivatives e.g. chloroquine
accumulate in parasite food vacuole and form cytotoxic complex with heme
Antifolates e.g. sulfonamides
target enzymes involved in folate synthesis required for parasite DNA synthesis
Antimicrobials e.g. tetracycline, doxycycline
target prokaryotic protein synthesis :. slow effect
Artemisinin derivatives e.g. artemether
binding iron and breaking down peroxide bridges
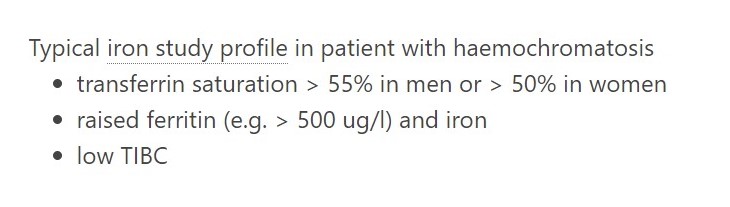
Name 2 iron tests that are most useful in monitoring haemochromatosis and why
Ferritin and transferrin saturation
Both tests can track response to treatment
Ferritin= measure of total iron stores
Transferrin saturation= measures how much serum iron is bound to the proteins in the blood
Briefly outline the differentials of acute chest pain for the main body systems
Cardiac- ACS, aortic dissection, pericarditis/myocarditis
Respiratory- PE, pneumothorax, pneumonia
GI- GORD, peptic ulcer disease, acute pancreatitis, oesophageal spasm/rupture
Other- MSK, shingles
Outline the features of complete heart block
Syncope
HF
Sinus bradycardia (30-50)
Wide pulse pressure (large difference between systolic and diastolic)
JVP
Variable intensity of S1
Briefly outline the treatment steps of angina
Aspirin + statin
GTN spray
BB or CCB
CCB monotherapy- verapamil or diltiazem (rate-limiting)
BB + CCB combination- amlodipine or modified-release nifedipine
Still symptomatic
long-acting nitrates e.g. ivabradine, nicorandil, ranolazine
PCI or CABG
Outline the NICE guidelines for diagnosing hypertension
Always ABPM to rule out ‘white coat HTN’
Which drugs should be taken for the secondary prevention of an MI?
BRATS
BB
Ramipril
Aspirin
Ticagrelor
Statin
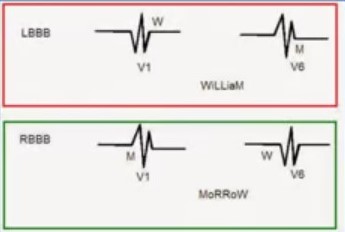
How do you identify RBBB and LBBB on an ECG?
LBBB: W in V1, M in V6
WiLLiaM
RBBB: M in V1, W in V6
MaRRoW
How do you differentiate between unstable angina and NSTEMI?
Both: ST depression and T wave inversion
Take troponin levels at 3hrs and 6hrs
IF ELEVATED→ NSTEMI
Normal troponin= unstable angina
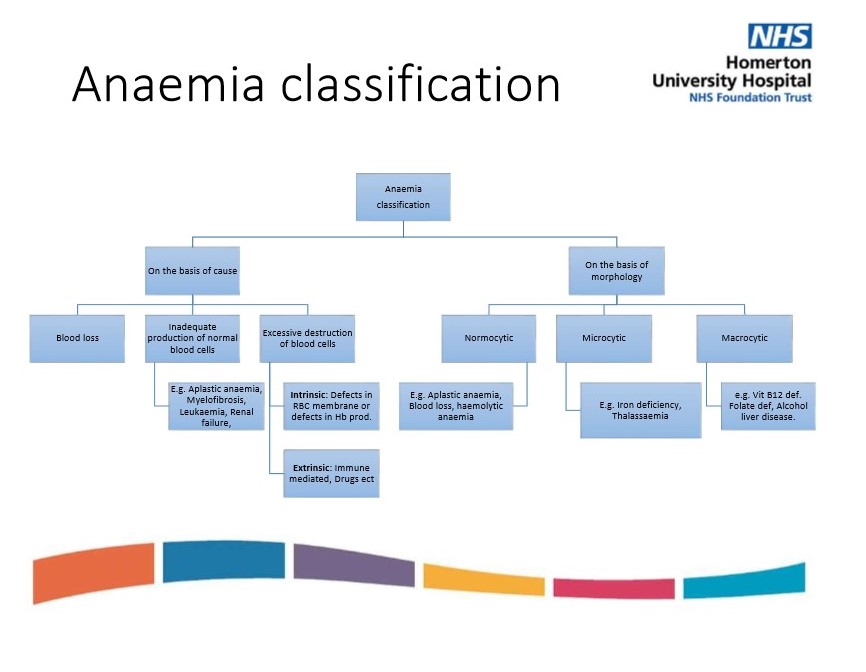
How is anemia classified?
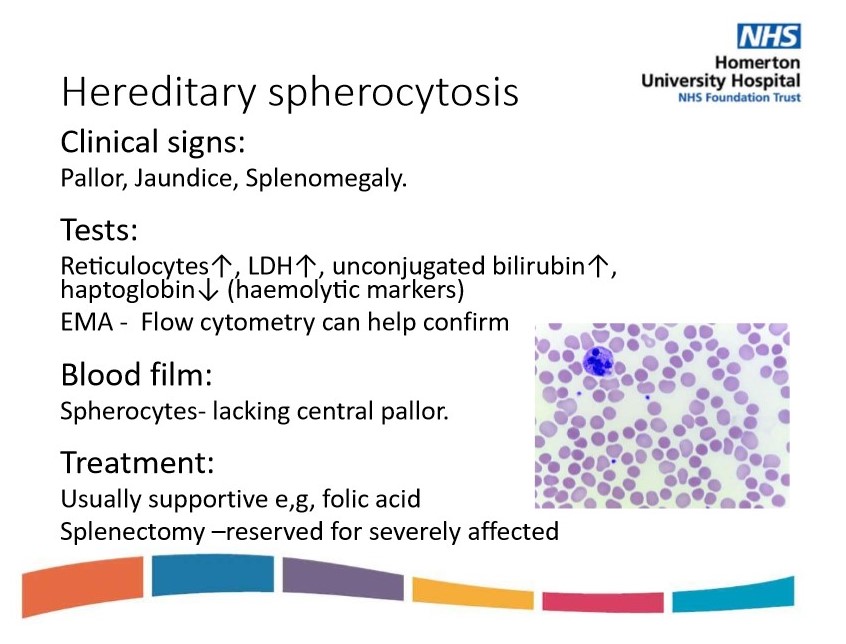
Describe hereditary spherocytosis- signs, tests, blood film and treatment
Genetic mutation resulting in defective RBC membrane
Usually hypochromic microcytic anemia
Increased destruction of RBCs
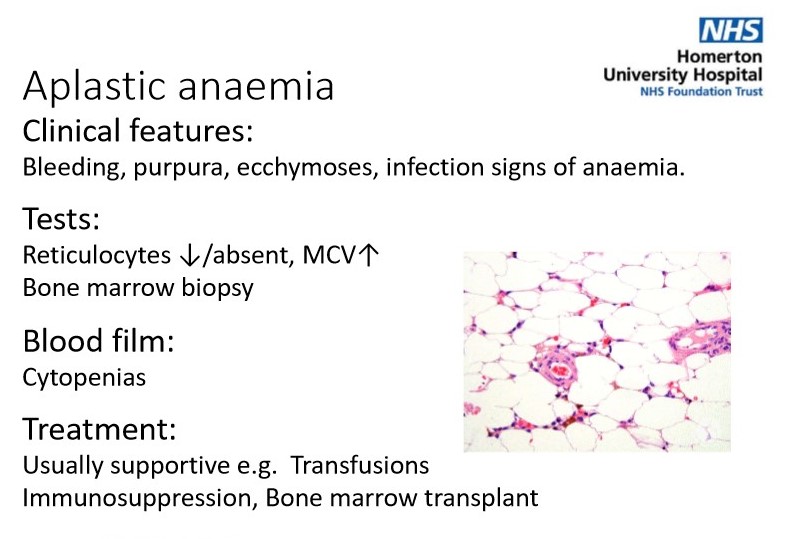
Describe aplastic anemia- clinical features, tests, blood film, treatment
Reduction or absence of hemopoietic precursors in all 3 cell lineages
Production issue
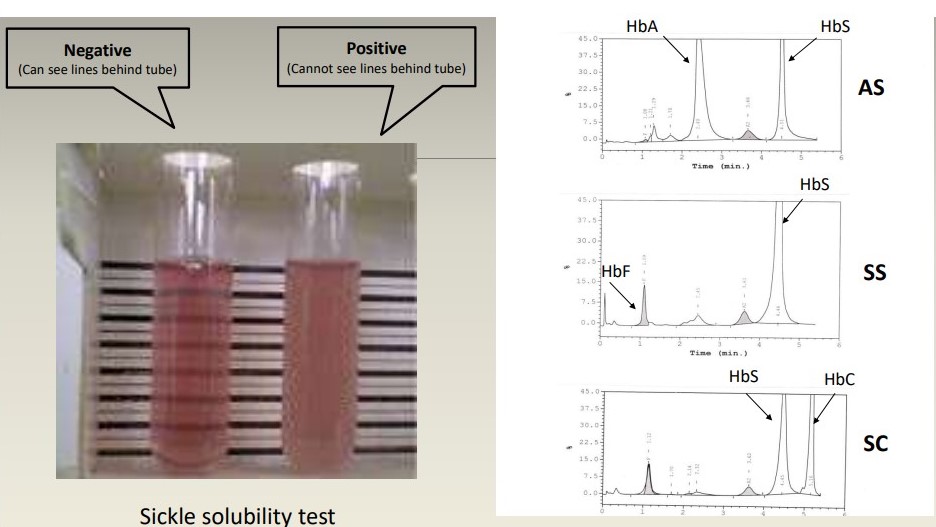
Outline the diagnosis of sickle cell disease
Clinical:
family history
recurrent pain
Lab:
FBC- anemia
haemolysis (high bilirubin, high LDH, raised reticulocytes, undetectable haptoglobin)
blood film
Hb electrophoresis/ sickle solubility test
Describe the emergency presentations of sickle cell disease
Briefly outline the 5 types of sickle cell crises
Thrombotic
AKA vaso-occlusive crisis
precipitated by infection, dehydration, deoxygenation
can occur in various organs e.g. bones, lungs, spleen, brain
Sequestration
sickling within organs e.g. spleen or lungs :. causes pooling of blood
associated with increased reticulocyte count
mainly in young children
Acute chest syndrome
VOC within pulmonary microvasculature :> infarction in lung parenchyma
SSx- SOB, chest pain, pulmonary infiltrates on CXR, low pO2
management- pain relief, O2, antibiotics, transfusion
Aplastic
infection with parvovirus (HPV B19)
sudden fall in Hb
bone marrow suppression causes reduced reticulocyte count
Haemolytic
rare
fall in Hb due to increased rate of haemolysis
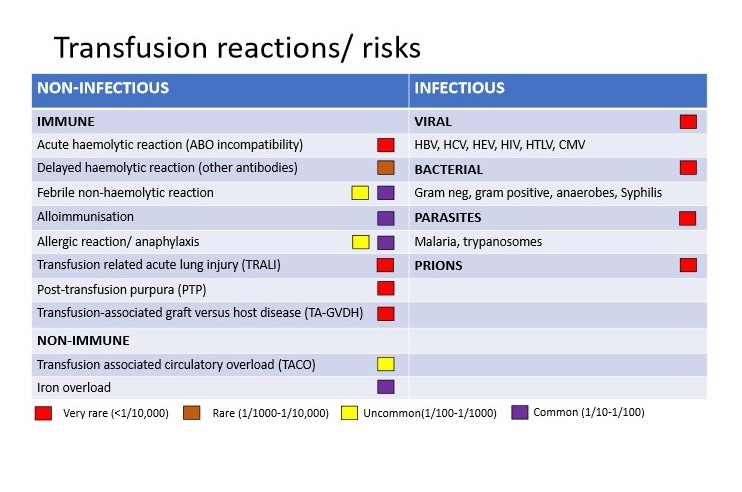
Briefly outline the main transfusion reactions
Acute haemolytic reaction
Delayed haemolytic reaction: 7-10 days after transfusion
Febrile non-haemolytic reaction: during or soon after transfusion
Anaphylaxis
TRALI: anti-leukocyte antibodies in donor react with recipient WBCs, within 6hrs
TACO: pulmonary oedema/respiratory compromise due to volume overload, within 12 hours
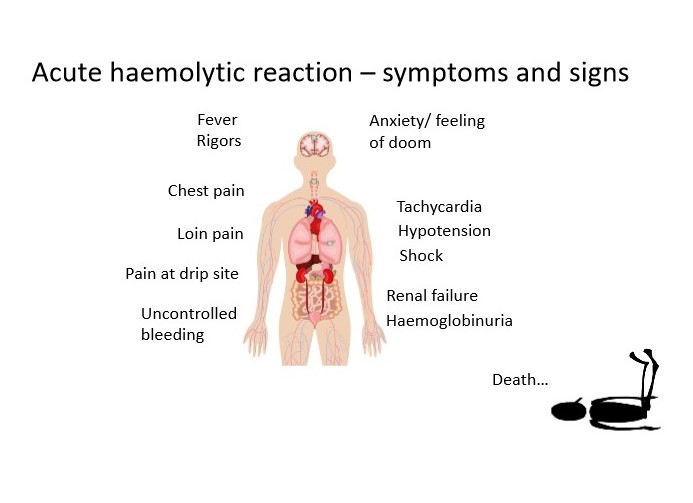
Outline the signs and symptoms of acute haemolytic reaction
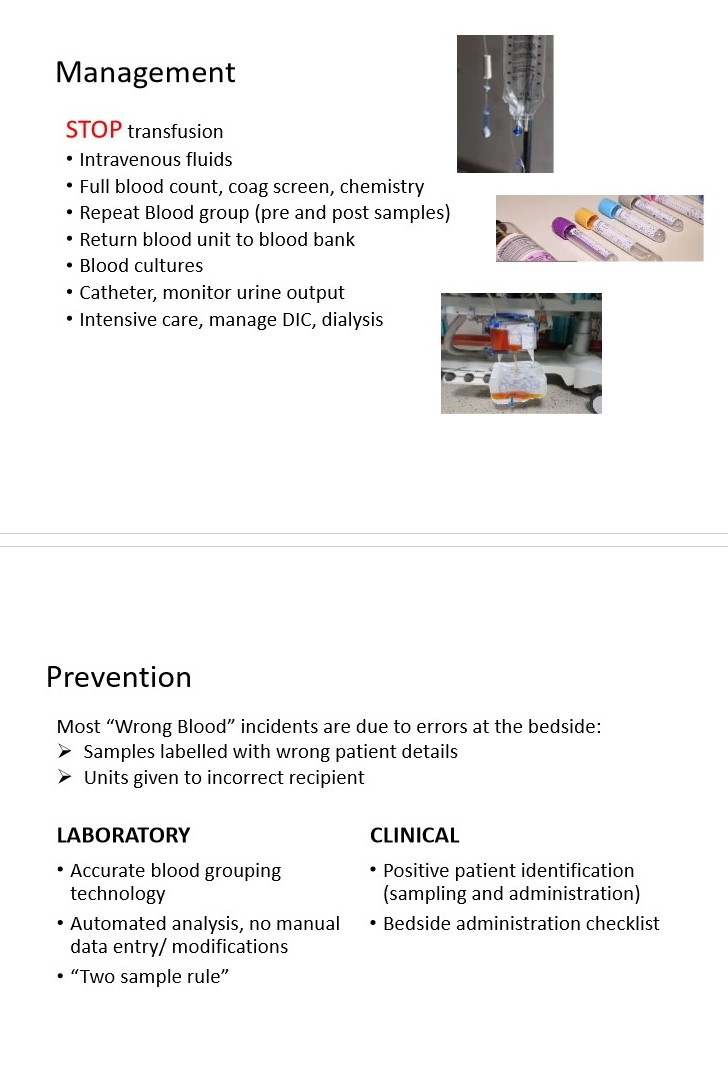
Outline the management and prevention of transfusion reactions
Outline how rheumatic fever typically presents
JONES criteria
Joints (arthritis)
O- carditis + pan-systolic murmur (looks like heart!!)
Nodules
Erythema marginatum (rash)
Sydenham’s chorea (late feature)- rapid, jerky, irregular movements
Outline the management of rheumatic fever
Oral penicillin IV
NSAIDs
Treat complications e.g. heart failure
Outline the features of hypercalcaemia
Bones, stones, groans and psychic moans
Corneal calcification
Shortened QT interval
HTN
Describe pulsus paradoxus
When there is an abnormally large drop in BP during inspiration
Usually presents in cardiac tamponade
Which artery is the preferred site for primary PCI?
Radial access
Next is Femoral
List 4 drugs recommended for reducing stroke risk in AF
DOACs e.g.
Apixaban
Dabigatran
Edoxaban
Rivaroxaban
Outline Takayasu’s arteritis- features, associations, investigation and management
Large vessel vasculitis
More common in younger females
Features: systemic features, unequal BP in upper limbs, absent/weak peripheral pulses, AR
Associations: renal artery stenosis
Investigations: magnetic resonance angiography (MRA) or CTA
Treatment: steroids
How does HOCM cause sudden death?
Ventricular tachycardia secondary to ischaemia
Occurs after extreme exertion
What are the echo findings in HOCM?
MR SAM ASH
Mitral regurgitation
Systolic anterior motion of the anterior mitral valve leaflet
Asymmetric hypertrophy
Briefly outline the main side effects of loop diuretics
Hypotension
Hypo→ Na+, Mg2+, Ca2+ and Cl-
Hyperglycaemia
Renal impairment
Ototoxicity
When is cardioversion used for AF?
If the patient is haemodynamically unstable
New onset AF that presents within 48hrs
lower risk of thrombus that could be dislodged
What is the first line management for a patient that is over 55yrs with stage 2 HTN and a QRISK score >10%?
CCB, statin and lifestyle advice
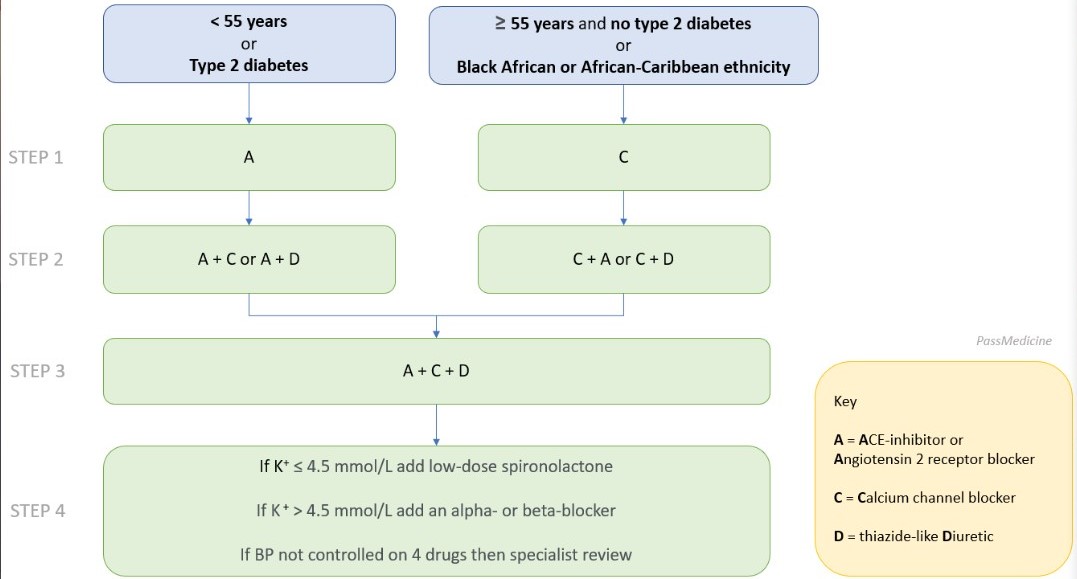
Outline the 4 steps of HTN management
1: A or C
2: A + C or A + D or C + D
3: A + C + D
4: K+< 4.5 → spironolactone
K+ > 4.5 → alpha or BB
Outline the management of HOCM
ABCDE
Amiodarone
Beta-blockers or verapamil for symptoms
Cardioverter defibrillator
Dual chamber pacemaker
Endocarditis prophylaxis
AVOID: nitrates, ACE-Is or inotropes (adrenaline, dobutamine)
Outline the secondary prevention of ACS
5A’s
Aspirin
And another antiplatelet
Atorvastatin
ACE-I/ARB
Atenolol (or other BB)
How are ACE-Is used in renal disease?
Should be stopped in AKI
They are reno-protective in CKD
Which biomarkers are most useful for confirming a reinfarction?
CK-MB: elevated 3-4 days following infarction
Troponin: elevated for 10 days following infarction
Outline the adverse effects of amiodarone
Indication: terminates SVT
chest pain
bronchospasm
transient flushing
Outline the management of acute NSTEMI
BATMAN
Beta blockers (unless contra-indicated)
Aspirin 300mg stat
Ticagrelor 180mg stat
Morphine
Anticoagulant (LMWH e.g. enoxaparin 1mg/kg)
Nitrates (GTN)
How should a patient with gout be treated for HTN?
ACE-I
if not controlled with ACE, add CCB over thiazide (even if low K+)
How does malignant hypertension typically present?
Severe HTN (>180 systolic)
Papilloedema
Retinal bleeding
Raised ICP
Which drug should patients be given before fibrinolysis?
Anti-thrombin drug e.g. fondaparinux
List the adverse effects of adenosine
Indication: terminates SVT
Chest pain
Bronchospasm
Transient flushing
Compare the ECG changes in bifascicular and trifascicular block
Bifascicular: RBBB and left axis deviation
Trifascicular: RBBB, left axis deviation and 1st degree heart block
Describe the ECG changes in hypothermia
Jesus Quist Its Bloody Freezing
J waves
QT interval prolonged
Irregular rhythm
Bradycardia
First degree heart block
Briefly outline the mechanism of warfarin
Oral anticoagulant used for VTE management + reducing stroke risk in AF
Inhibits epoxide reductase preventing the reduction of vitamin K to its active hydroquinone form
:. acts as a cofactor for clotting factor II, VII, IX and X (1972) and protein C
Taking warfarin increases INR :. takes longer for blood to clot
List the warfarin inducers
Inducers: decrease INR (increase effect of warfarin)
SCARS
Smoking
Chronic alcohol intake
Antiepileptics (phenytoin, carbamazepine, barbiturates)
Rifampicin
St. John’s Wort
List the inhibitors of warfarin
Inhibitors: cause increase in INR (counter effect of warfarin)
ASS-ZOLES
Antibiotics (ciprofloxacin, erythromycin, isoniazid, clarithromycin)
SSRIs
Sodium valproate
Zoles- omeprazole, ketoconazole, fluconazole
When should amiodarone be used?
Pharmacological cardioversion of AF if there is structural heart disease
Typically more chronic AF
Which ECG abnormality is commonly seen in hypercalcaemia?
Short QT interval
Painful bones, renal stones, abdominal groans and psychic moans