Process of moving the fetus, placenta and membranes out of the birth canal
Labor
First stage of labor
onset of regular contractions to full dilation of cervix
second stage of labor
full dilation to delivery of baby
third stage of labor
delivery of baby to delivery of placenta
fourth stage of labpr
delivery of placenta to first 4 hours after birth
Impending signs of approaching labour involve a variety of physiological and psychological signs. Like:
Lightening (fetal engagement) \n Braxton Hicks contractions \n Bloody Show \n Backache \n Spontaneous Rupture of membranes (SROM)
Diarrhea \n Spurt of energy (nesting) \n Weight loss
True or False labor: Contractions are regular and close together
true
true or false labor: contractions are irregular and not occurring closer together
false
How would change in activity affect true labor vs false labor
True labor: Contractions continue no matter if comfort measures.
False labor: Contractions may stop or slow down with comfort measures
cervical changes in true vs false labor:
true labor: Progressive dilatation & effacement.
false labor: Cervix may be soft but no sign in change in effacement or dilation and no show
True or false labor:Contraction discomfort is Usually felt in the front of the abdomen. May be felt in the back
false
true or false labor: contraction discomfort Starts in the back and radiates towards the front of the abdomen
true
contraction strength of true labor
becomes stronger with time; vaginal pressure is felt
contraction strength of false labor
freq weak; not getting stronger with time
what are the P’s of labor
Power
Passageway
passenger
position
Psychological response
Powers
Primary – Involuntary uterine contractions that result in Effacement and Dilatation of the cervix
Secondary – Involuntary urge to push
average primiparous woman dilates __ cm / hr
1
average multiparous woman dilates __ cm / hr
1.5
Passageway
Refers to Maternal Pelvis
-Structures,
-Types (shape),
-Diameter, -
and Soft tissues
-“Give” of joints –effect of hormones
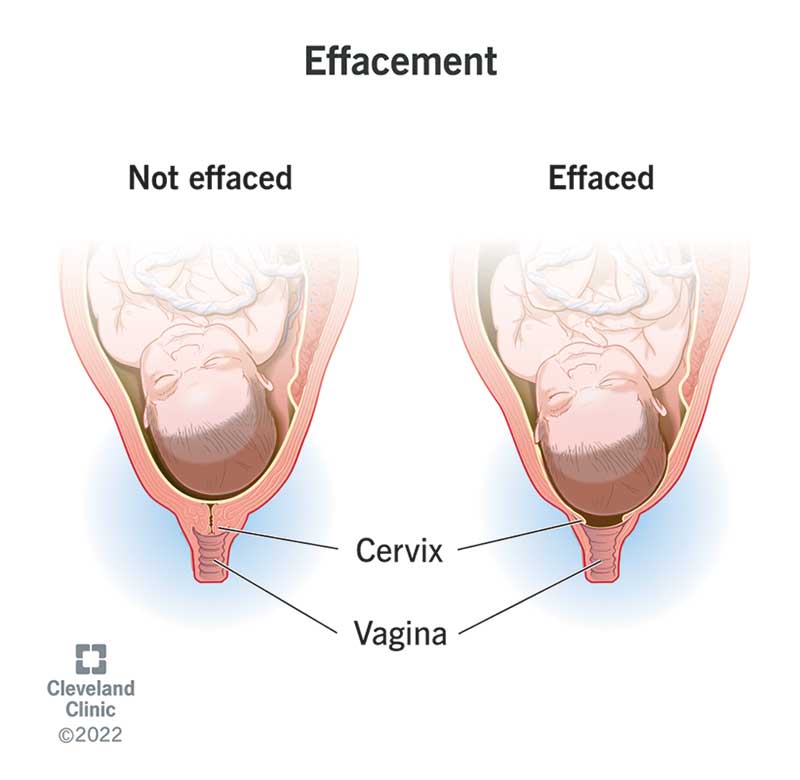
Effacement
the cervix stretches and gets thinner
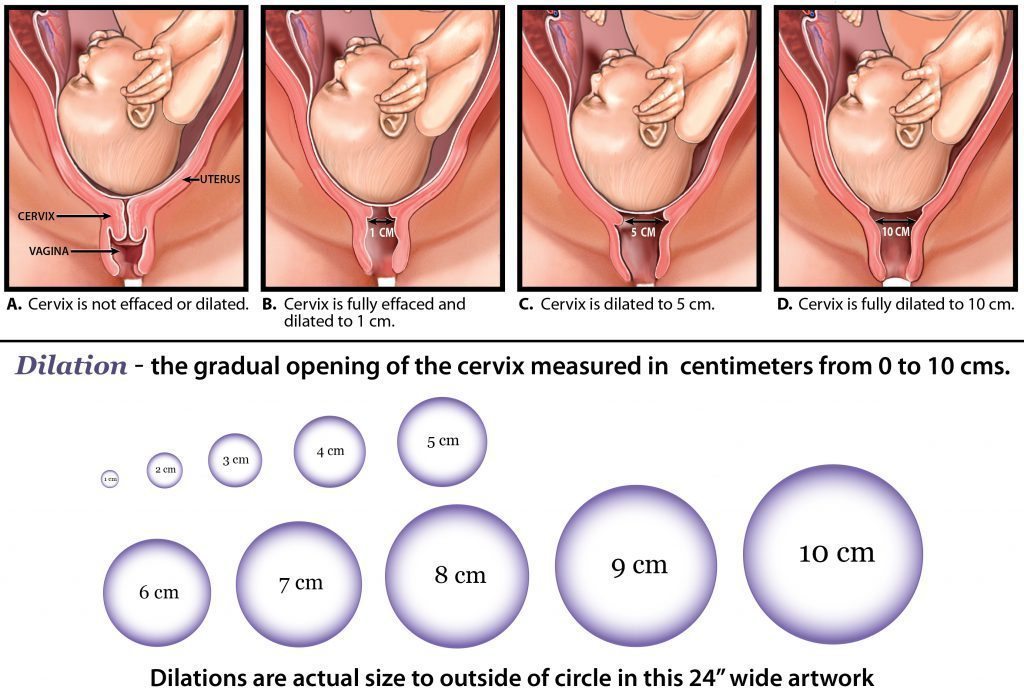
dilation
Dilatation means that the cervix opens
passenger
Fetal head – dimensions
Cranial Vault (Bones)
Sutures (sagittal/lambdoidal/coronal)
Fontanelles \n Biparietal diameter
*Fontanelles/ \n sutures and fetal head positioning are important mechanisms to aid in passing through the maternal pelvis
fetal lie
Fetal lie refers to the relationship between the longitudinal axis of the baby with respect to the longitudinal axis of the mother (longitudinal lie, transverse lie, oblique lie)
fetal presentation
Fetal presentation refers to the part of the baby that is overlying the maternal pelvis.
fetal presenting part
the presenting part is the part of the baby that leads the way through the birth canal. Most often, it is the baby's head, but it can be a shoulder, the buttocks, or the feet.
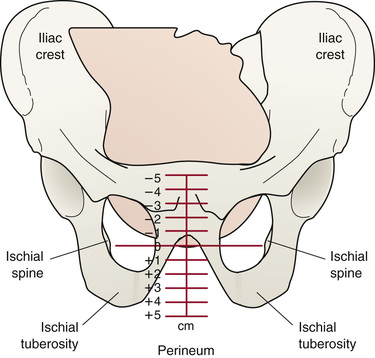
fetal station
Station is the relationship of the presenting fetal part to an imaginary line drawn between the maternal ischial spines and is a measure of the degree of descent of the presenting part of the fetus through the birth canal.
Engagement
Engagement is the term used to indicate that the largest transverse diameter of the presenting part (usually the biparietal diameter) has passed through the maternal pelvic brim or 405inlet into the true pelvis and usually corresponds to station 0. Engagement often occurs in the weeks just before labour begins in nulliparas and may occur before or during labour in multiparas. Engagement can be determined by abdominal or vaginal examination.
friedman’s curve
Relationship between cervical E&D and fetal descent in relation to time and progression of labour
lateral position improves
circulation
hands and knees position makes
fetus rotate
squatting position does what
opens the pelvis
what stage is labor: is the process of effacement (%) and dilation (cm) of the cervix
first
what are the 3 phases of the first stage of labor
latent, active, transition
latent phase of first stage takes how long?
7-8 hours
how much dilated are they in latent stage
0-3cm
how long are contractions in the latent phase of phase 1
30-45 seconds
how long is the active phase in the first stage of labor
3-5 hours
how far dilated are they in the active stage
4-7cm
what % effaced in the active stage
40-80%
how long are contractions in the active stage of the first stage
40-60 seconds in length
how many cm dilated in the transition stage
8-10cm
how long is the transition stage
30 min - 2 hrs
what % effaced in the transition phase
80-100%
how long are contractions in the transition phase
60-90 seconds
first stage physical assessment
-Vaginal examination- to determine the progress of labour (cervical effacement and dilation)
- Uterine activity- Contractions pattern and strength
- Bloody show
- Amniotic fluid
- Comfort level
-Vital signs
- Fetal assessment – fetal heart rate patterns
- Leopolds manoeuvres
-Hydration status
- Bowel, bladder status
rupture of membranes there will be a presence of ______ in amniotic fluid
sodium chloride
what if rupture of membranes is green amniotic fluid
-meconium stained amniotic fluid.
-Meconium in the amniotic fluid increases the risk for meconium aspiration syndrome.
Endotracheal intubation and suctioning in infants who
are not vigorous at birth should occur prior to drying and stimulation to remove any meconium from the trachea.
stage 1 latent phase nursing interventions :
Contractions – Q 30 -45 sec duration, mild to mod, 5 – 20 min apart
Encourage mobility, change positions frequently
Encourage voiding q2h
Maintain adequate hydration/ diet
Support/ comfort measures
Monitoring of labour progress and fetal adaptation to labour stress
Maternal positioning that facilitates descent of the fetus and comfort for the labouring person
what part of the first stage of labor is this:
Contractions- Q 2- 4 min apart, moderate to strong, 60 seconds duration.
Progression of emotional display as labour progresses
active phase
active phase of labor nursing interventions
-Continue with latent phase interventions (mobility, positioning, voiding, hydration, etc... )
-Monitor comfort/pain management – pain becomes more intense during this phase
-Fetal monitoring and assessment – important to note how fetus is responding to labour progress
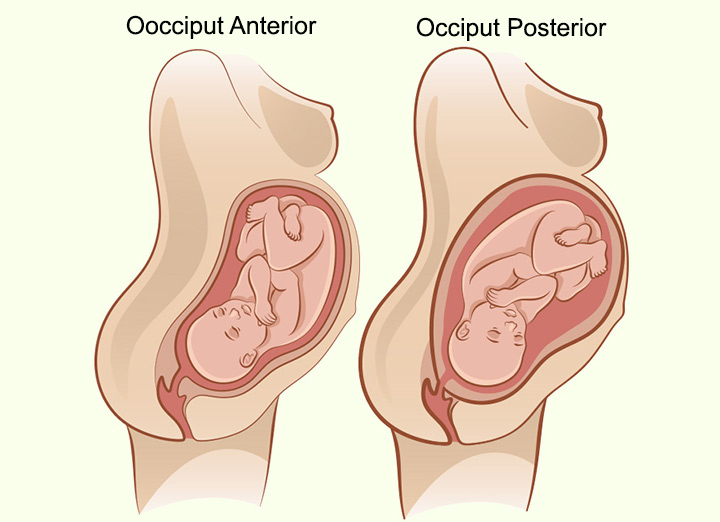
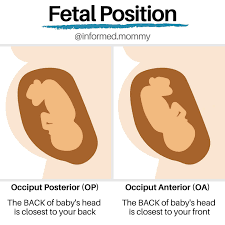
Op position during labor is a lot of
back pain
OP vs OA position
effleurage
(non pharm pain management)
a form of massage involving a circular stroking movement made with the palm of the hand.
transition stage contractions
70-90 secs in duration.
strong.
30-60 seconds apart
transition phase nursing care
-Emotional support +++/positive reinforcement. May need frequent focus and direction
- Help control breathing through contractions \n -Begin to get for delivery
- Prepare bed and positioning for pushing
childbirth \n - Pharmacologic Pain control may be too late at
this point (respiratory effects on neonate)
induction of labor is a common intervention during the ____ stage of labor
first
what is induction of labor
artificial initiation of labor
important considerations prior to induction of labour
Bishop Score System -Measures cervical readiness for induction by scoring 5 characteristics of the cervix 5 characteristics include:
1. Dilation (5 cm or more) 2. Effacement (80% or more) 3. Station (+1 or more ) 4. Cervical consistency (firm, medium, soft) 5. Cervical Position (Posterior, midposition, anterior**)
why would induction of labour be required
Post term infant
Diagnosed issue of intrauterine environment
ie.) perfusion of fetus
Fetal distress (if not severe) or risk for fetal
distress identified.
augmentation
labor has started but it needs help
why would augmentation of labour be reuired
-Supplementation of a naturally occurring labour with synthetic oxytocin. \n • Purpose would be to increase the strength/
pattern or duration of contractions to improve the labour process.
post term pregnancy continues past the end of the ____ completed weeks of gestation
41
risks of post term labor on mother
-tears/lacerations
-Labour dystocia
-Increased risk of infection and hemorrhage
risk of post term labor on infant
Meconium aspiration
Infant injury from birthing process
Mortality rate increases after 40 weeks
methods of cervical ripening
Natural endogenous oxytocin release:
• Sexual intercourse
Mechanical methods: \n • Amniotomy \n • Stripping or sweeping of membranes
Pharmacologic methods:
• Prostaglandins \n • Oxytocin
synthetic prostaglandins (PGE2)
Frequently used to ripen the cervix.
Cervix has to be ripened for labour to be initiated. If bishop score is less than 6, a cervical ripening agent such as prostaglandins must be used before labour induction.
If cervix is not ripened, augmentation or induction with oxytocin will not be successful
synthetic oxytocin
• Synthetic form of the naturally occurring hormone
• Used to facilitate uterine contractions \n • Can be used to induce labour or augment labour
• Piggybacked into main IV infusion line
and titrated until regular contraction pattern is established
nursing care for oxytocin induction
• V/S q30mins (BP &P) and on increase of drip
• Record FHR & contractions q15mins \n • Monitor contractions closely
• If fetal distress- \n -d/c oxytocin, increase main line \n -turn on left side \n -administer oxygen \n -reevaluate contractions and fetal response -notify doctor \n -document
second stage of labor Phases:
-initial latent phase
-descent (cardinal ,ovements)
-active expulsion phase (pushing and crowning)
how long is the second stage of labor
lasts up to 1 hour
from complete dilation (10 cm) to birth of the newborn
second stage of labor
physiological s/s of full dilation (2nd stage of labor)
Sudden appearance of sweat on upper lip
Vomiting episode \n Increase in bloody show
Increased restlessness/agitation ;
verbalization – “I cant go on”
Involuntary bearing down efforts
Bulging perineum, labia
7 cardinal movements
-Descent \n -Flexion \n - Internal Rotation
- Extension
- Restitution \n - External Rotation
- Expulsion
when is apgar scoring done
1 min after birth and 5 mins
what degree tear? involves fourchette, perineal skin, vaginal mucous membrane without involving any muscles.
first
what degree tear? muscles of perineum
second
what degree tear? also extends to rectal sphincter
third
what degree tear?also extends into rectum
fourth
third stage of labor is the separation and delivery of the placenta. usually takes ? mins after birth of baby
5-30
signs of separation of placenta in the 3rd stage of labor
-Firmly contracting uterus
- Change in shape of uterus from discoid
to globular
- Lengthening of cord \n - Sudden gush of blood \n -Vaginal fullness or membranes at the
introitus
what is the baby side of the placenta
shiny schultz
maternal side of placenta
dirty duncan
when is the placenta considered retained?
30 mins after delivery… not good if its still there
fourth stage of labor
1- 4 hr after birth of the newborn; period of maternal physiological adjustment.
-Restoration of physiology \n -Myometrial contractions and retractions & vessel thrombosis \n -BLEEDING MAIN CONCERN \n -Formation of mother-newborn relationship
-Consolidation of family unit
the golden hour
undisturbed first hour after birth spent skin to skin on mother’s (or father’s) chest, unclothed
Many benefit for infant as well as mother’s transition to postpartum period
Facilitates bonding and attachment
Promotes regulation of newborns physiological
transitions to extra uterine life (Eases transition period)
Allows mother to adjust to puerperium stage physically and emotionally
Preterm labour is true labour that begins before __ completed weeks of gestation
37
premature rupture of membranes (PROM)
rupture or membranes prior to onset of labour regardless of gestational age
Preterm PROM (pPROM) – rupture of membranes before 37 weeks gestation
Predisposing factors- maternal nutritional deficiencies, substance use, placental abruption, polyhydramnios, multiple pregnancy, prior preterm birth or PPROM, infections **primarily chorioamnionitis or trauma
Once membranes rupture - risk of infection- chorioamnionitis. Usually caused by normal flora e.g. E coli
care for PROM
Restrict activity with ongoing assessment.
Ie) Temp at least Q2hr together with WBC and CBC
monitoring daily. Admin of broad spectrum antibiotics
• Try to prevent infection- no pv exams, frequent changing of pads, observe amniotic fluid for signs of infection, tachycardia in baby, adequate hydration
most women will go into labor within 24hr of PROM. but if not, ______ is necessary if they are over 37 weeks (not preterm)
induction
Prom.
if fetal distress or infection..
induce right away
cervical insufficiency
-Generally painless cervical dilation \n -Often associated with pPROM and preterm birth
-Risk Factors: Excessive cervical dilation for curettage or biopsy, history of previous cervical lacerations during childbirth, cervical and uterine anomalies, a hx of short labours and/or losses at early gestations
-TX: Cerclage, Restricted Activity (potentially bedrest)
-Placed at 13 – 14 weeks and removed at 37 weeks gestation
suppressing premature labor
Bedrest – left lateral
incraesed hydration so increased plasma volume
Avoid unnecessary pv exams
Tocolytics
Corticosteroids- betamethasone/dexamethasone•
Continuous monitoring of FHR and contractions
Needs lots of psychological support
dystocia
long, difficult, or abnormal labor
criteria for dystocia
4 hours of < 0.5 cm/hr dilation (active first
phase)
\n OR
1 hr with no descent while pushing (second stage)
failure to progress
(dystocia)
cervix does not dilate despite normal uterine contraction and no CPD
hypotonic labor
-Unable to dilate cervix normally \n -Uterus is easily indented at peak of contraction \n -Usually occurs in active phase of First Stage \n -Possible causes: Uterine overdistention, fetal malposition, analgesics, regional anaesthesia
management of hypotonic labor
If membranes intact and presenting part is engaged – amninotomy and/or oxytocin augmentation
hypertonic labor
Possible cause may be synthetic oxytocin ,hyperstimulation, or placental abruption
Usually occurs in latent phase in the first stage of labor
Management:
Rest
Fluids
Sedation/ analgesia
No oxytocin (Stop infusion -Short half life)
Occurs when the uterus never fully relaxes between contractions.
Contractions are erratic and poorly co-ordinated
Cervix doesn’t dilate as normal (labour prolonged)
Placental Perfusion is compromised; Fetal oxygenation is reduced
hypertonic labor
FDI
frequency, duration, intensity
(of contractions)